









Introduction
Hydatidosis is a zoonosis caused by the larval form of a cestode of the species Echinococcus granulosus, the canine tapeworm. Humans can be an accidental intermediate host [1]. Hydatidosis is widespread throughout the world, especially the Mediterranean area, East Europe, South America, the Middle East, East Africa, and Australia [2].
Echinococcosis can affect any organ of the human body except nails, hair, and cornea [3]. It most often involves the liver (63%), lungs (25%), muscles (5%), and bones (5%) [4]. Involvement of organs in the small pelvis is extremely rare, at 0.2–2.25% of cases [5], mainly secondary to dissemination of hydatidosis from another organ [6–14].
In the small pelvis, the ovaries are most often involved (80%), followed by the uterus [5, 15].
We present a case of secondary echinococcosis in the pelvis, simultaneously involving the left ovary and the uterus.
Case report
We present a 41-year-old Caucasian woman, gravida 1, without accompanying diseases, who came to the clinic with complaints of mild pain, heaviness in the small pelvis, and a fibroid detected by ultrasound examination. In amenorrhoea for 3 months. An intramural nodule measuring 39/45 mm and a septated cyst of the left ovary 44/40 mm were found from the ultrasound examination. From the anamnesis, she reported that in 1997 she was operated on urgently due to an acute abdomen, and it turned out that she had a ruptured echinococcal cyst of the liver. During the operation, 2 additional echinococcal cysts were found between the intestinal loops, which were removed together with the right adnexa.
In 2013, due to acute abdominal pain and a diagnosis of acute appendicitis, she was operated on again. One echinococcal cyst was found in the region of sigmoid epiploic appendages, reactively inflamed appendix, and myomatous enlarged uterus. The appendix and the echinococcus cyst were removed.
A computed tomography scan of the abdomen and pelvis was performed, and cystic formations were found in the liver and pelvis (Fig. 1).
Fig. 1
Computed tomography scan findings: old hepatic echinococcal cysts – at the border of the left/right liver lobe a separated cystic lesion, in places with calcium inclusions in the wall 42/27 mm and in the right lobe paracaval devitalized echinococcal cyst 21/16 mm (A), calcifications subcapsular 10/5 mm (B), intramural fibroid node 39/30 mm (C), lesion with calcium density in the right parauterine 12/9 mm (D), in the area of the left ovary, a hyperdense, separated lesion with calcium deposits 44/31/41 mm (E), cyst formation in the uterine wall 29/24 mm (F)
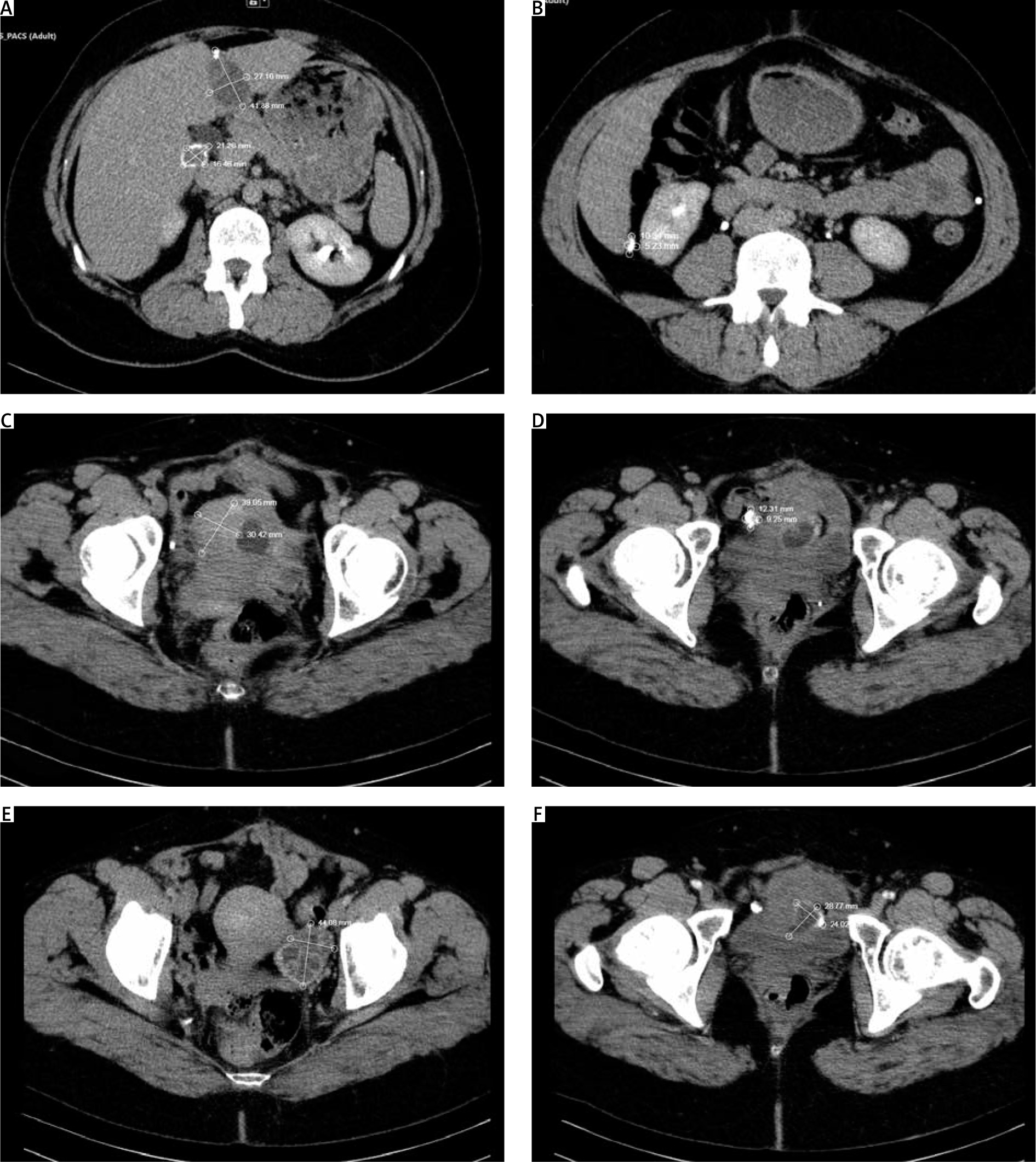
As a result of the performed imaging studies, it was decided that it is about old single calcified echinococcal cysts in the liver and a suspected recurrence with a new cyst in a small pelvis – both in the ovary and uterus.
Echinococcal IgG antibodies were tested with ELISA – 0.5 (negative result). The results of the full blood count and biochemistry were normal.
An abdominal total hysterectomy with left adnexectomy was performed (Fig. 2).

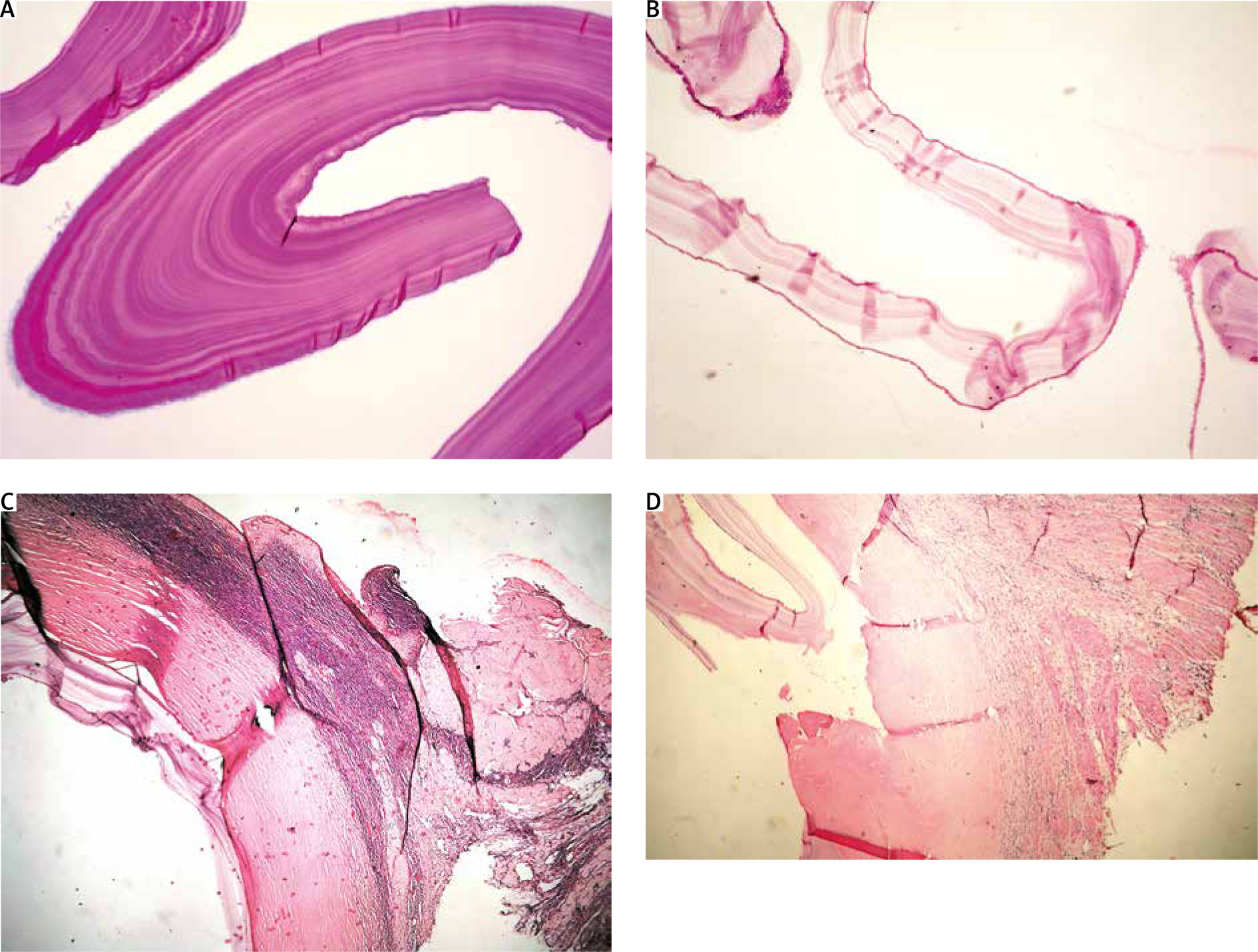
The histological result was as follows: basal endometrium and myometrium with endometriosis, leiomyoma nodes with secondary changes, 2 echinococcal cysts PAS (+), ovarian parenchyma with white bodies, fibrous cyst wall with calcium deposits, lined with chitin membrane PAS (+) (Fig. 3).
Fig. 3
Histological findings: ovarian parenchyma with white bodies, fibrous cyst wall with adjacent chitinous membrane – 40×, H and E (A), chitin membrane with germ layer – 100×, H and E (B), chitin membrane with germ layer – 100×, PAS (C), myometrium with fibrous cyst wall with adjacent chitinous membrane with germ layer – 40×, H and E (D)
The patient was discharged on the 4th postoperative day without complications. One year later, there is no evidence of recurrence of echinococcosis.
Discussion
Each year, between 2 and 3 million cases of human echinococcosis are observed worldwide [16]. Endemic areas are the Middle East, the southern part of South America, Iceland, Australia, New Zealand, southern parts of Africa, Central Asia, and China [3]. Echinococcus granulosus usually affects a single organ and presents as a slowly growing (0.5–3 cm per year), noninvasive, unilocular cystic lesion [3]. In 10–15% of cases it affects 2 organs [17]. Pelvic involvement is rare (0.3–0.9%), with 80% involving the genitalia, and the ovaries being more commonly involved than the uterus [3]. This usually occurs secondarily to intra-abdominal rupture of a hydatid cyst of the liver, although cases of primary uterine involvement have also been described [18].
The clinical picture of pelvic echinococcosis is nonspecific: abdominal swelling, abdominal pain, menstrual abnormalities, infertility, and urinary disturbances [9]. Ovarian or uterine echinococcosis can mimic polycystic ovaries or malignancy [10, 11], multicystic ovarian tumour, haemorrhagic ovarian cyst, endometrioma, cystadenoma, leiomyoma, etc. [19, 20].
The diagnosis is supported by ultrasound examination or computed tomography (CT) scan because the images do not have specific characteristics [11]. The anamnesis is of utmost importance because it can lead the doctor to think about this disease. Early diagnosis is very important because it allows the surgeon to prepare for operative treatment, which is the gold standard of treatment. The surgeon must avoid intraoperative iatrogenic rupture, which can lead to anaphylactic shock, and when necessary, pre-administer albendazole-based therapy to reduce the risk of spread, which can lead to relapses [12]. Surgical treatment can be radical (removal of the cyst with the affected organ) or conservative (removal of the cyst only) [2]. If impossible, the cyst can be aspirated and marsupialized [4].
In our case, the diagnosis was made after the ultrasound examination, due to the previous history of 2 surgical interventions in the abdomen for echinococcosis.
Our patient presented with nonspecific complaints of pain and heaviness, but despite this, a decision was made to perform a hysterectomy with left adnexectomy due to the presence of a cystic formation in the uterus, which was detected on CT. In this case, it is a case of secondary echinococcosis (both in the ovary and uterus), which occurred most likely as a result of a previous rupture of a liver cyst.
As far as we know, this is the second case described in the literature with echinococcosis being found simultaneously in the uterus and ovary. The first case was from 1969 and was described in Bulgaria [21].
Only a few cases with primary fallopian tube involvement are reported in the literature – less than 30 [22]. Usually, they are diagnosed during surgery or as paraovarian cysts [23, 24].
The involvement of the uterus is another rare location of echinococcosis, and it can occur primarily or secondarily [3]. It was reported for the first time by Gueddana in 1990 [25], and there are no specific diagnostic symptoms.
From the female reproductive organs, hydatidosis occurs most often in the ovaries, and it can be a primary or secondary disease [2].
Conclusions
In patients with a positive history of previous echinococcosis, especially in endemic areas, echinococcosis should be considered as a possible cause of pelvic mass. Diagnosing this disease is extremely important for proper treatment. As rare as uterine involvement is, this possibility should not be overlooked.