





Supraglottic airway devices (SADs) play an important role in management of difficult airways due to easy insertion with continuous patient ventilation [1–3].
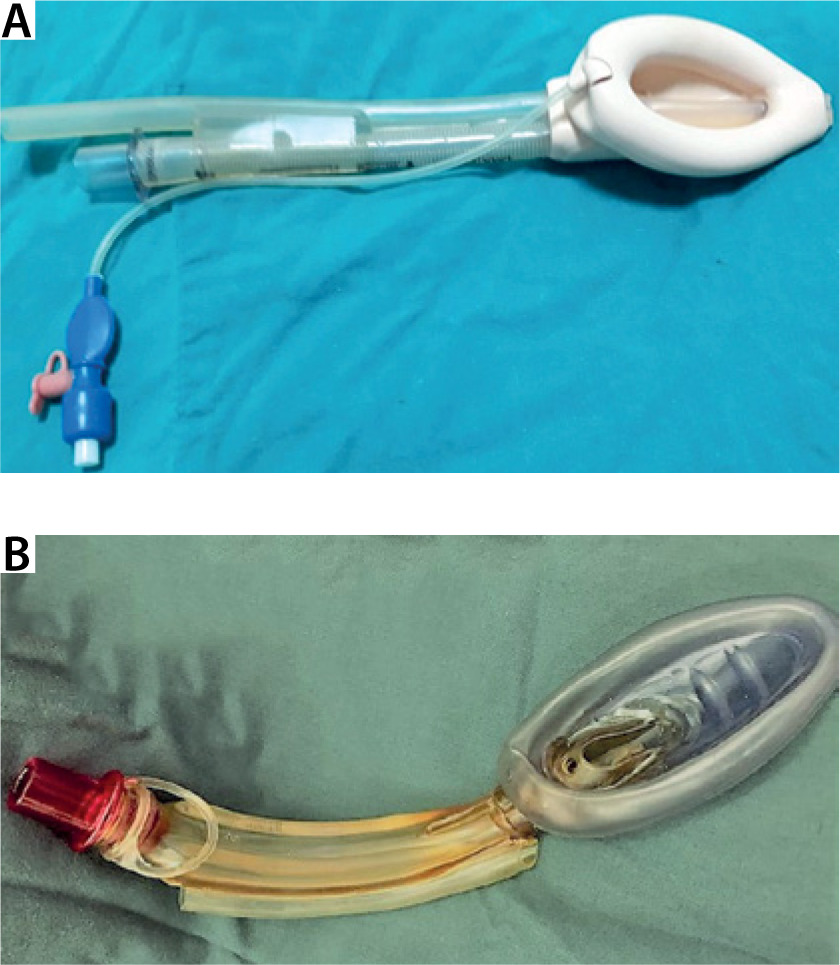
The Proseal Laryngeal Mask Airway (PLMA) (Fig-ure 1A) is a reusable silicon-based SAD that has a drainage channel and a redesigned cuff. This device is considered a second-generation SAD and is designed to facilitate a gastric tube passage and prevent gastric insufflation, hence enhancing its safety. The airway tube is equipped with a bite block. The selection of the PLMA size is based on the patient’s weight, with size 3 recommended for those weighing 30–50 kg, size 4 for those weighing 50–70 kg, and size 5 for those weighing 70–100 kg. In order to obtain an intra-cuff pressure of 60 cmH2O, the cuff of the PLMA should be inflated with an appropriate amount of air, which may be measured using a portable cuff manometer [4].
The Air-Q Self Pressurized Airway Device with Blocker tube in place (SP Blocker) (Figure 1B) is a new self-pressurizing disposable PVC (polyvinyl chloride)-made SAD. It functions as a standard Air-Q device because it maintains a flexible perimeter mask cuff, which enhances its ability to adjust the form and size of the cuff according to the patient’s pharyngeal architecture. SP Blocker incorporates a large aperture between its breathing tube and cuff, resulting in automatic cuff self-pressurizing to proper inflation pressure with cyclical reduction of intra-cuff pressure in order to reduce nerve and mucosal damage. It has an integrated bite block and a new separate built-in soft flexible guide tube that can accept either a regular gastric tube, blocker tube or suction tube. This tube is a large-bore, multi-orifice drain tube that is designed to pass through the guide channel for accessing and suctioning the posterior pharynx in addition to suctioning, venting, and blocking the upper esophagus. SP Blocker size selection is dependent on the patient’s weight (size 2.5: 30–50 kg; size 3.5: 50–70 kg; size 4.5: 70–100 kg) [5].
FIGURE 1
Proseal Laryngeal Mask Airway (PLMA) (A) and Air-Q Self Pressurized Airway Device with Blocker (SP Blocker) (B)
Our research evaluated the efficiency of the PLMA and the SP Blocker during positive pressure ventilation (PPV) in female patients undergoing elective gynecological operations. The primary outcome (OLP) and secondary outcomes (peak inspiratory pressure [PIP], OLP-PIP, ventilation score, fiber-optic glottis view score, dynamic lung compliance [Cdyn], airway resistance [Raw] and ventilatory parameters which included inspired tidal volume [ITV], expired tidal volume [ETV], leak volume [LV] and leak fraction [LF]) were recorded initially after confirmed successful SAD insertion with adequate ventilation, then at five predefined time points (5, 15, 30, 45 and 60 minutes) after SAD insertion.
METHODS
This study was performed in the gynecological unit of Cairo University Hospitals and is a prospective, randomized, controlled, two-arm parallel trial.
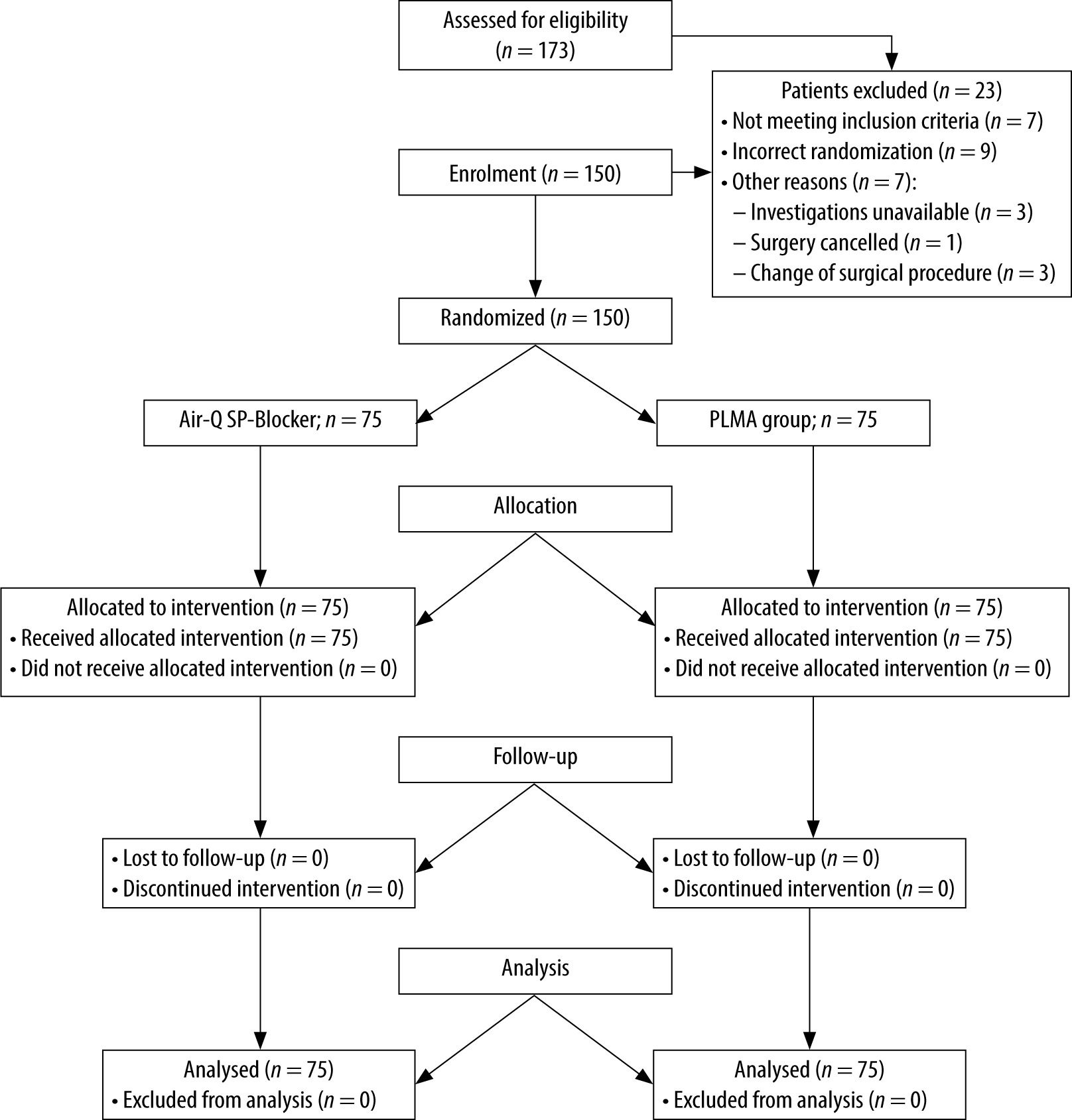
Firstly, ethical approval was obtained in 2017 (Ethical Committee N-95-2017), then secondly updated in 2024(Ethical Committee N-188-2024) by Research Ethical Committee of Cairo University Hospitals. The study was registered at https://clinicaltrials.gov/NCT03384056 on the 14th of December 2017 by the principal investigator, Reham Ali Abdelrahman, before patients’ enrollment. Thereafter, written informed consent was obtained from all participants before enrollment. This study was performed in compliance with the applicable Equator guidelines as the recruitment of participants was done according to the Consort flow chart diagram (Figure 2).
We included in the study adult female patients scheduled for elective gynecological surgery. Patients with an El-Ganzouri score of five or less, those with upper airway issues, those with a hiatus hernia, pregnant women, and those with obstructive sleep apnea were excluded.
The eligible participants were recruited in a sequential manner and then randomly assigned to either the PLMA group or the SP Blocker group using an online randomization application (http://www.randomizer.org) with an allocation ratio of 1 : 1. Concealment was effectively achieved by using opaque, sealed envelopes that were sequentially numbered. The investigator, denoted as N.E., who had the randomization information, did not participate in any experimental procedures.
General anesthesia was achieved with propofol 2 mg kg–1 and fentanyl 1 µg kg–1. After confirming loss of consciousness, rocuronium 0.3 mg kg–1 was administered [6]. Mask ventilation was continued using 3–4 vol% of sevoflurane for 3 min. When muscle relaxation was attained (train-of-four [TOF] = 0), the chosen device, lubricated with water-soluble jelly, was inserted in the patient’s mouth by the principal investigator (R.A.), who performed 40 successful SP-Blocker insertions in addition to 200 prior PLMA insertions.
PLMA group: a size 4 device with a deflated cuff was inserted in the subsequent cuff and the sniffing position was inflated with just enough air to achieve an intra-cuff pressure of 60 cmH2O, which was maintained by regular check of the cuff every 20 minutes until surgery, terminated through removing extra air from the cuff by a syringe. The PLMA was preloaded with a 16 Fr. gastric tube.
SP Blocker group: a size 3.5 device was inserted in the extended neck position by opening the patient’s mouth and elevating the tongue with a tongue blade to lift the epiglottis off the posterior pharyngeal wall to allow easy passage into the pharynx until fixed resistance to forward movement was felt. The blocker tube was inserted into the esophagus after correct device placement.
A maximum of 2 attempts were allowed for each patient. The first selection of the size of the SAD was determined by the weight of the patient. In cases where ventilation became insufficient, as indicated by a suboptimal capnographic curve and/or the delivery of an inadequate tidal volume resulting in a fractional loss exceeding 20% of the predetermined tidal volume, various manipulations were allowed. These manipulations were categorized into two categories: major and minor. Minor interventions encompassed adjustments of the position of the head and neck, modifications to the depth of insertion through gentle pushing or pulling of the SAD, jaw thrust, and chin lift. Major interventions involved re-insertion of the SAD or changing its size.
The term “effective ventilation” was operationally defined as a capnograph trace exhibiting a square-wave pattern, accompanied by a plateau and bilateral symmetrical chest movement observed during manual ventilation. This was achieved by gently squeezing the reservoir bag while ensuring the absence of any audible gas escape. A failed attempt was defined as device removal before its re-insertion. If the SAD could not be inserted by the second attempt, tracheal intubation was performed and the participant was excluded from the study. After confirming successful SAD placement, PPV was applied using pressure regulated volume control mode (PRVC) with a tidal volume of 8 mL kg–1 of predicted body weight, initial ventilator rate of 12 breaths min–1, adjusted to maintain ETCO2 in the range 35–40 mmHg, I : E ratio: 1 : 2, and a rate of gas flow 4 L min–1.
Anesthesia targeted a bispectral index of 40–60 was achieved using sevoflurane with FIO2 0.4, anal-gesia, by intravenous (IV) pethidine 0.5 mg kg–1, while muscle relaxation (guided by peripheral nerve stimulator) was maintained with intermittent boluses of rocuronium 0.1 mg kg–1. The SAD was removed along with its drain tube after confirming adequate spontaneous respiration. Postoperatively paracetamol 1 g as IV infusion was repeated every 6 hours.
Primary outcome: oropharyngeal leak pressure (OLP) (cmH2O): The observed leak sound around the lips during apnea was indicative of the reached plateau pressure when the adjustable pressure-limiting valve of the circle system was fully closed and fresh gas flow of 3 L min–1 was maintained. In order to prioritize safety, the maximum allowed operating pressure (OLP) was established at 40 cmH2O [7–9].
Secondary outcomes:
Peak inspiratory pressure (cmH2O).
OLP-PIP (cmH2O).
Dynamic lung compliance (Cdyn) (mL cmH2O–1).
Resistance of airway (Raw) (cmH2O L–1 s–1).
The ventilatory parameters, including inspired tidal volume, expired tidal volume, leak volume and leak fraction LF, were documented. The formula for calculating the load factor (LF) as a percentage is derived from the equation LV = ITV – ETV. The load factor is determined by dividing LV by ITV and multiplying the result by 100 [10, 11]. The airway sealing quality score was used to assess the degree of leak (Table 1) [12].
The Brimacombe fiber-optic glottis view score method was used to evaluate the fitting of SADs in relation to the laryngeal aperture. This assessment was conducted using a flexible fiber-optic bronchoscope, which was inserted through the airway tube of the SAD while the head was maintained in a neutral posture. The results of this evaluation can be seen in Table 2. The Brimacombe scores of 4 or 3 were considered to be good, whereas scores of 2, 1, or 0 were considered negative. When the examination of bronchoscopy reveals the presence of the esophageal aperture, it is advisable to re-insert the device [13–15].
The ventilation score was determined by three criteria: the absence of leakage at an airway pressure of 15 cmH2O, the presence of bilateral chest excursions at a PIP of 20 cmH2O, and the observation of a square wave capnogram. Each criterion was assigned a value of either 0 or 1 point. When all three conditions were met, the ventilation score was determined to be 3 [6, 9, 16–18].
Insertion variables:
The insertion time, measured in seconds, refers to the duration required for the accurate installation of SADs. This time interval starts when the SAD makes contact with the teeth and ends at the point when the first recorded rectangular capnogram curve is observed, accompanied with adequate bilateral chest expansion [9]. Only successful efforts were taken into consideration.
The ease of inserting SADs is assessed using a four-point scoring system. A score of 3 indicates successful insertion on the first try without encountering any tactile resistance. A score of 2 indicates successful insertion on the first attempt, but with some tactile resistance. A score of 1 indicates successful insertion on the second attempt. A score of 0 indicates unsuccessful insertion on the second attempt [12, 19, 20].
The study data included the time required for the insertion of drain tubes, namely the blocker tube in the SP Blocker and the stomach tube in the PLMA. Additionally, the number of attempts made during the insertion process was recorded. The success of tube placement was assessed using a three-point scale, where a score of 1 indicated ease of installation, a score of 2 indicated difficulty and a score of 3 indicated impossibility of placement. Failure was defined as the lack of successful tube insertion within a maximum of two attempts [21].
Perioperative variables:
Duration of: anesthesia induction (s), mechanical ventilation (min), emergence (s), unassisted spontaneous ventilation duration (s), duration of surgical procedure (min), SpO2 (%), ETCO2 (mmHg), intra-operative blood-gas samples and haemodynamic parameters.
Laryngopharyngeal morbidity (LPM) parameters noted 1 and 4 hours postoperatively (Table 3) [18, 20].
TABLE 1
Quality score of airway sealing [12]
TABLE 2
TABLE 3
Statistical analysis
Student’s t-test was used to examine continuous variables that followed a normal distribution. The data were presented as mean and standard deviation. The determination of normality for continuous variables among groups was conducted using the Shapiro-Wilk test. The analysis of categorical variables included the use of the chi-squared test, with the resulting data being presented in terms of sample size number and percentage (n, %). The Kruskal-Wallis test, a non-parametric method for comparing different groups, was used to analyze the hemodynamic data. To further examine the differences between groups, a Dunn multiple comparison test was conducted. The statistical analysis was performed using the SPSS program (IBM SPSS Statistics, version 25). The statistical tests were conducted with a confidence range of 95% (α-error = 0.05) and a research power of 80% (β-error = 0.2). P-values less than 0.05 were considered statistically significant.
Sample size calculation
Our main hypothesis posited that OLP was the most precise indicator of SADs’ effectiveness. The design of our research was adequately powered to assess the superiority of the SP Blocker compared to the PLMA for the treatment of OLP. The authors obtained pilot data before to conduct this investigation on the SP Blocker, which revealed a mean OLP of 29 cmH2O with a standard deviation (SD) of 6.33 cmH2O. In contrast, the published values for the ProSeal Laryngeal Mask Airway were 25.9 cmH2O with an SD of 5.2 cmH2O [22]. When evaluating the clinical significance of the difference in OLP between SP Blocker and PLMA devices, we determined that a difference of 3.1 cmH2O is the lowest value considered to be relevant. This difference was obtained by subtracting the OLP of the PLMA (25.9 cmH2O) from the OLP of the SP Blocker (29 cmH2O). To further analyze this difference, we calculated a standardized difference (d) by dividing the target difference (3.1 cmH2O) by the standard deviation (SD) of 6.33. The resulting standardized difference was 0.49 (3.1/6.33). The Altman nomogram can be utilized to perform a two-sample comparison of a continuous variable. This nomogram allows for the determination of the required number of subjects in each group, based on the standardized difference, power, and significance level. The formula used is n = (2/d2) × Cp, where n represents the number of subjects required in each group, d is the standardized difference, and Cp is a constant determined by the chosen values for the P-value and power [23, 24]. In order to facilitate ease of analysis, it was postulated that the two groups should possess equal proportions.
In this investigation, the critical power (Cp) was determined to be C0.05, 80% = 7.9. Based on this value, it was determined that a minimum of 66 participants would be needed in each group. The calculation for this sample size was performed using the formula n = 2/(0.49)2 x 7.9, resulting in n = (2/0.24) x 7.9 = 66. To account for any dropouts, the sample size was extended to 73 by adding 10% (n/(1 – 0.1) = 66/0.9 = 73). The authors included a total of 75 patients per group in order to determine a significance level of 5%. The estimated minimum sample size required to achieve a statistical power of 80% and a two-sided alpha level of 0.05, in order to detect a standardized difference of 0.49, was around 150.
RESULTS
From February, 2018 to November, 2019, 173 patients were randomly tested for eligibility. Twenty-three patients were excluded, so that a total of 150 patients were included in the final analysis and divided into 75 patients in each group (Figure 2) that showed no variance regarding demographic data (Table 4), peri-operative variables (Table 5), LPM score at 1 and 4 hours postoperatively (Table 6), and insertion variables with the exception of a significantly shorter insertion time of the SP Blocker than the PLMA (Table 7).
TABLE 4
Comparison between Air-Q SP Blocker and Proseal Laryngeal Mask Airway regarding demographic data
TABLE 5
Comparison between Air-Q SP-Blocker and PLMA regarding perioperative variables
TABLE 6
Comparison between Air-Q SP Blocker and PLMA regarding laryngopharyngeal morbidity parameters
TABLE 7
Comparison between Air-Q SP Blocker and Proseal Laryngeal Mask Airway regarding insertion variables
At insertion, the SP Blocker group showed statistically significantly higher mean OLP, lower mean PIP, higher mean (OLP-PIP), higher mean ITV, higher mean ETV, lower mean LV, lower mean LF, better fiber-optic glottis view score and higher mean Cdyn than the PLMA group, but both groups showed no statistically significant difference regarding airway resistance and ventilation score (Table 8).
TABLE 8
Comparison between Air-Q SP Blocker and Proseal Laryngeal Mask Airway regarding performance parameters immediately after insertion
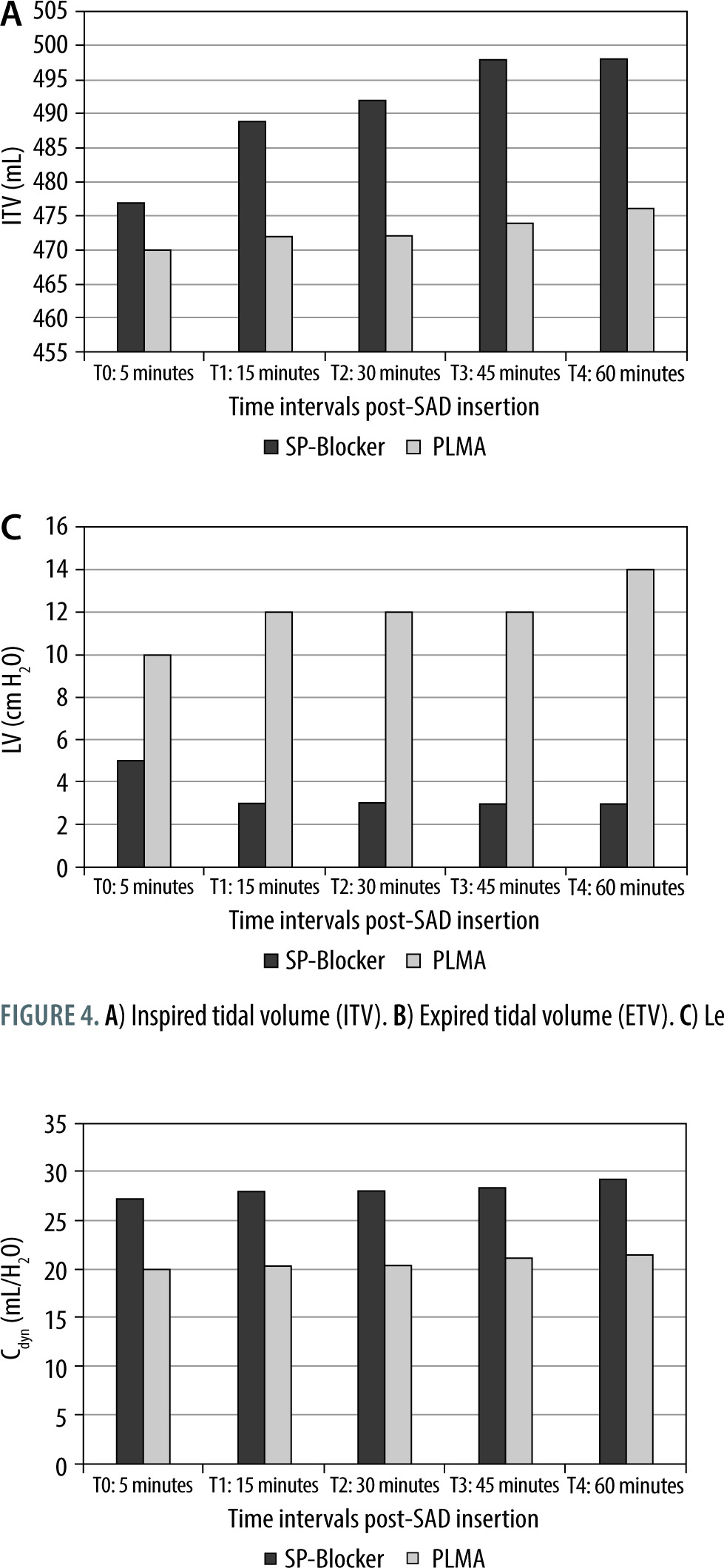
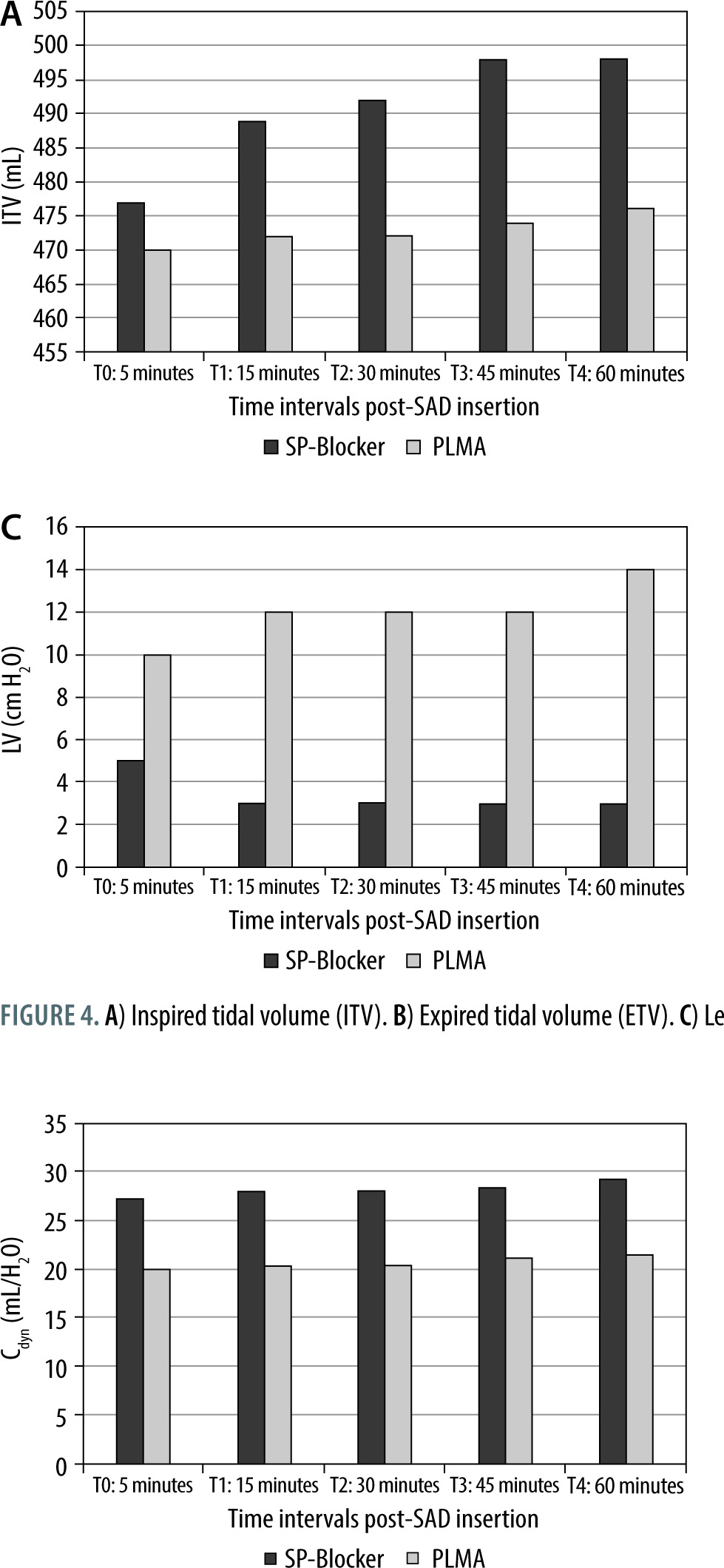
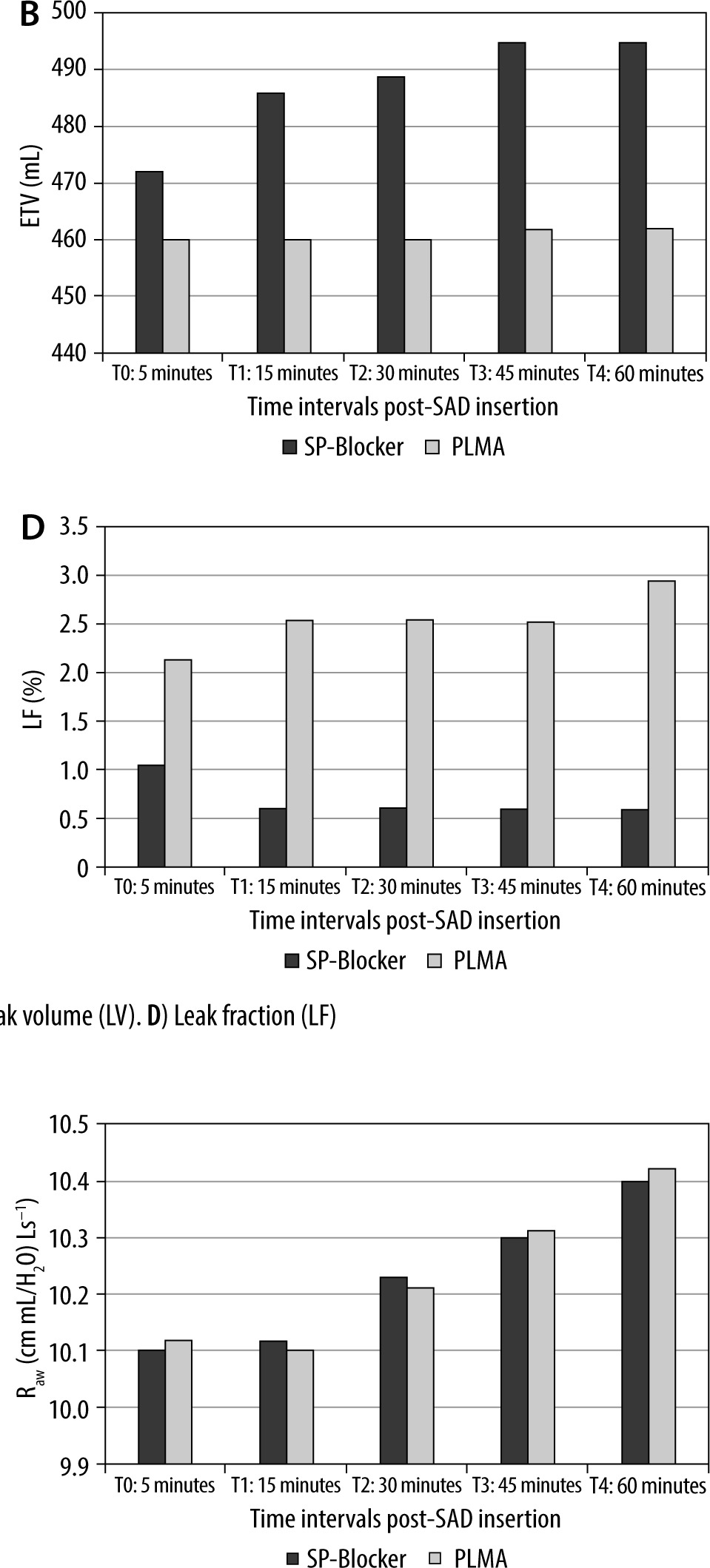
At five predefined time points (5, 15, 30, 45 and 60 minutes) after successful SAD insertion the SP Blocker group showed statistically significantly higher mean OLP (Figure 3A), lower mean PIP (Figure 3B), higher mean (OLP-PIP) (Figure 3C), higher mean ITV (Figure 4A), higher mean ETV (Figure 4B), lower mean LV (Figure 4C), and lower mean LF (Figure 4D) than the PLMA group. Throughout the ope-rative time the SP Blocker offered significantly higher Cdyn (Figure 5) than the PLMA without any significant changes in the airway resistance (Figure 6).
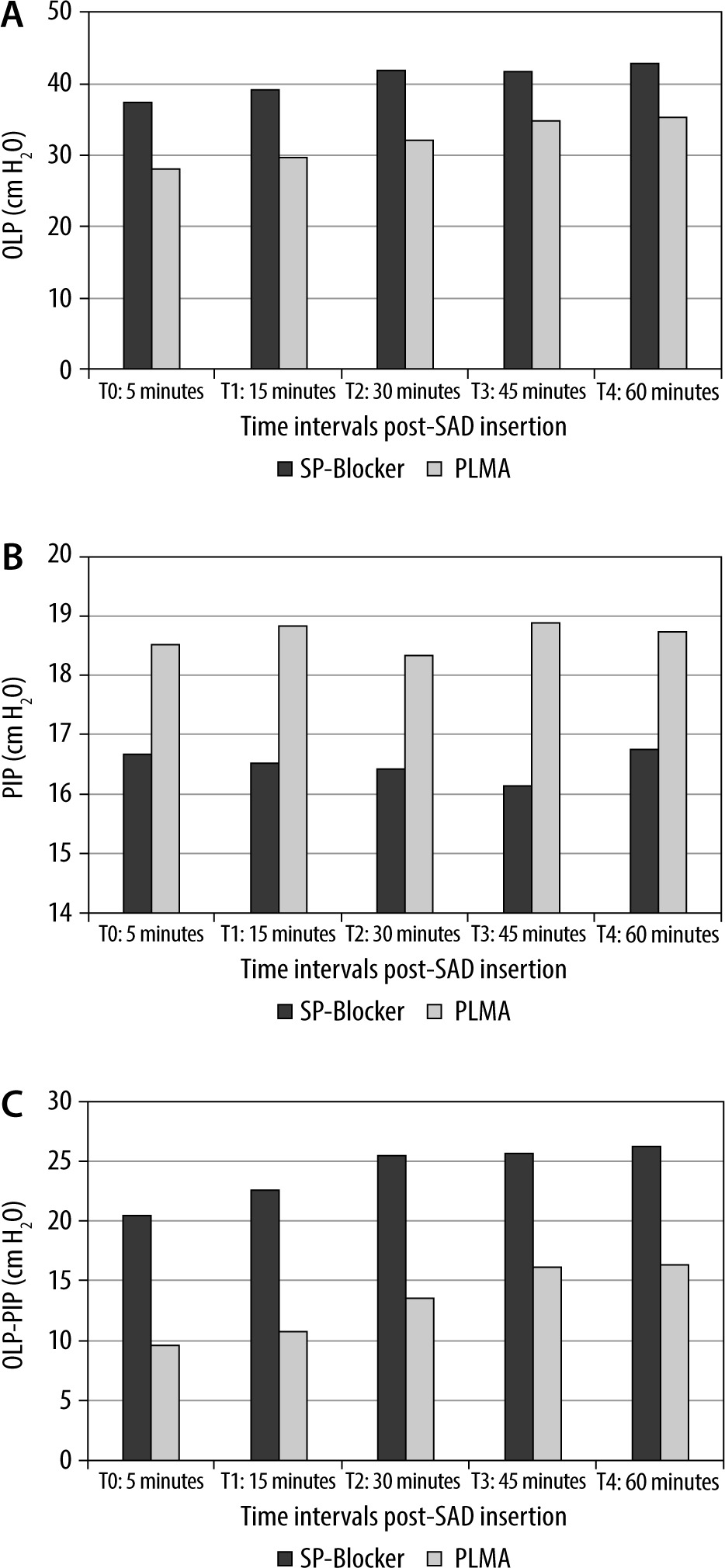
FIGURE 4
A) Inspired tidal volume (ITV). B) Expired tidal volume (ETV). C) Leak volume (LV). D) Leak fraction (LF)
Data were expressed as number (%) or average ± SD and a P-value < 0.05 was considered significant.
DISCUSSION
SADs are safer than face masks due to provision of a glottis seal [25]. The Air-Q family has included the standard Air-Q (Air-Q ILA), Air-Q Blocker and Air-Q SP [26–33]. The SP Blocker is an enhanced disposable PVC-made version of the standard Air-Q representing a revolution in SADs design [5, 34]. The PLMA is a reusable silicone-made SAD that can provide a better glottis seal permitting use of high airway pressures without leak [35–37]. Our discussion was based on SP Blocker functions similarly to the standard Air-Q.
The present study demonstrated that the SP Blocker had a more effective clinical performance than PLMA, while patients kept in a neutral position in the absence of intra-abdominal contents displacement, through provision of higher OLP, lower PIP, higher ITV and ETV, lower LV and LF, and higher Cdyn with a better fiber-optic glottis view score.
Although the PLMA is constructed from silicone, which conforms adequately to supraglottic structures better than PVC, with intra-cuff pressure maintained at 60 cmH2O, a significantly higher OLP was found in the SP Blocker group due to the better seal provided by the non-inflatable cuff of the SP Blocker beside its unique design features: the anterior curve of its airway tube that approximates the oropharyngeal airway providing stable end-to-end coupling with the glottis, mask ridges that stabilize the bowl transversely and higher posterior heel height that improves the seal at the tongue [38, 39]. Our results clinically corroborate two studies showing that the mean OLP of the Air-Q Blocker and Air-Q SP became higher than that of the PLMA, but they did not agree with a study which found that Air-Q ILA has a lower mean OLP than the PLMA, while previous studies found no statistically significant differences when comparing either the Air-Q ILA and the PLMA or the Air-Q Blocker and the PLMA [6, 31, 40–42].
As the SP Blocker is molded to the posterior pharynx with better alignment of its ventilating orifice to the laryngeal inlet resulting in significant increase in OLP throughout the surgery more than PLMA, this could explain the significant increase in ITV and ETV with subsequently a significant decrease in LV and LF with the SP Blocker compared to the PLMA. Our observation agreed with a study by Beleña et al. [11] which confirmed that higher OLP was consistent with achievement of higher tidal volumes and other studies reported that the significant reduction in OLP in the extended neck position resulted in significant reduction in tidal volumes when using the Air-Q SP airway or PLMA, but contrasted with a previous study which found no difference between the Air-Q ILA and PLMA with respect to ventilatory parameters in spite of lower OLP with the Air-Q ILA than the PLMA [8, 42, 43].
Although the investigators emphasized ade-quate anesthetic depth in both groups, in addition to low tidal volume ventilation using the PRVC mode, which according to Ghabach et al. [44] is advantageous over volume controlled ventilation in reducing PIP and increasing Cdyn, the SP Blocker group presented significantly lower PIP and higher Cdyn than the PLMA group, and this could be attri-buted to the SP Blocker design, which offered less resistive load than the PLMA design.
However, the disposable SP Blocker has a short wide airway tube in comparison to the reusable PLMA. It appears to be stiffer and less flexible due to the physical properties of the rigid high density PVC (phthalate-free)-made SP Blocker compared to the soft silicone-made PLMA, making the SP Blocker more resistant to gas pressure, and this might be the nullifying factor accounting for similar Raw in both groups.
In our study the SP Blocker was found to have a shorter insertion time than the PLMA because the SP Blocker is devoid of an inflatable cuff, in contrast to the PLMA, which needed time to inflate its cuff and adjust its volume. Our result was in line with research proving that the pre-curved stiffer PVC-made Air-Q or SP Air-Q took less time to insert when compared with silicon-made devices such as the PLMA that resulted in higher friction against the tongue, palatal and hypopharyngeal mucosa [45–47]. This showed that the 40 prior SP Blocker insertions were valuable for its perfect placement. However, it should be noted that the shorter insertion time of SP Blocker by 2 seconds when compared to the PLMA may not be important except when SAD insertion is preceded by an interval of hypoxia.
However, no significant differences existed between the compared groups regarding ease of SAD insertion and the first-attempt insertion success rate. Our results were consistent with previous comparisons such as Air-Q ILA versus PLMA, Air-Q SP versus PLMA and Air-Q Blocker versus PLMA, which rated similar ease of insertion and first-attempt insertion success rate within each compared group but with a significantly shorter insertion time of the Air-Q ILA, Air-Q SP and Air-Q Blocker than the PLMA [26, 31, 41]. However, our trial was at odds with another comparison between the Air-Q Blocker and the PLMA by Gupta et al. [40] which revealed a shorter insertion time and a higher success rate of insertion for the first time with better ease of insertion in the PLMA group than the Air-Q Blocker group, while Moorthy et al. [42] found no significant difference between the Air-Q ILA and PLMA regarding insertion time, ease and attempts of insertion. Easy insertion of the SP Blocker is consistent with a previous study showing easy insertion of the Air-Q, but in contrast to another report documenting that the Air-Q SP became more difficult to place despite its shorter insertion time [28, 32]. The SP Blocker was as successfully placed at the first attempt as the Air-Q ILA and Air-Q SP [48–50].
The improved design of the SP Blocker, including a keyhole-shaped ventilating orifice for resting epiglottis and raised heel of the mask cuff, can ele-vate the epiglottis and center larynx, maximizing space for the fiber-optic bronchoscope resulting in a better view of the laryngeal inlet with the SP Blocker than the PLMA, and this finding was in agreement with studies examining the standard Air-Q which reported a better fiber-optic view when the Air-Q was compared with first generation SADs and second generation SADs, but at odds with studies which found no difference in fiber-optic glottis view when comparing the Air-Q Blocker vs. the PLMA and the Air-Q ILA vs. the PLMA [26, 31, 32, 41, 42, 48–57].
Both groups showed insignificant low incidence of LPM symptoms at 1 and 4 hours postoperatively, and this is attributed to decreased risk of cuff over-inflation in the SP Blocker group with subsequently less pressure exerted on the pharyngeal wall, minimizing airway morbidities. Furthermore, the intra-cuff pressure of the PLMA was maintained at 60 cmH2O throughout the study. These results agree with Youssef et al. [31], Gupta et al. [40], Aly et al. [41] and Moorthy et al. [42], but contrast with another study comparing the Air-Q ILA and PLMA which documented significant LPM symptoms in the Air-Q group compared to the PLMA group – mainly gross blood on the device at its removal and throat pain in the recovery area with pain on swallowing at 24 h follow-up [26].
Regarding hemodynamics, our data were recorded at different time points and showed no statistically significant differences between groups and even within each group, the recordings showing minimal insignificant cardiovascular changes as was found previously by Youssef et al. [31], and Hwang et al. [33]. However, Gupta et al. [40] found that heart rate (HR), mean (MBP) diastolic (DBP), and systolic blood pressure (SBP) values were comparable and insignificant when the Air-Q Blocker was compared with the PLMA, except during the first 5 minutes immediately after Air-Q Blocker insertion when there was a greater rise in blood pressures than with the PLMA. However, Galgon et al. [26], who compared the Air-Q ILA and PLMA, recording hemodynamic and respiratory data at baseline and over the first 5 min following device placement, observed insignificant changes over time regarding HR and SpO2 that were similar to our results, but in contrast to our observations SBP, DBP and MBP decreased over time in both groups with values that became significantly higher in the Air-Q ILA than the PLMA group.
Concerning performance of the related drain tube (blocker tube for SP Blocker/gastric tube for PLMA), no statistically significant difference was found between the compared devices in addition to complete absence of gastric insufflation in both groups. Our findings are in contrast to a study by Gupta et al. [40]. They recorded a significant difference between the success rate of insertion of the blocker tube in the Air-Q Blocker versus the gastric tube (16 Fr) in the PLMA, where the whole PLMA group was successfully preloaded with its gastric tube with successful stomach evacuation in contrast to the Air-Q Blocker group as the blocker tube could not be passed in 4 patients and in 2 of them the stomach could not be evacuated and the device was replaced with an endotracheal tube. Moreover, a previous study comparing the Air-Q SP versus the Supreme showed two cases in the Air-Q SP group with vomiting and gastric insufflation as there was no suction hole and suction was often applied after device removal [58]. Our study demonstrated the importance of the new separate built-in soft flexible guide tube of the SP Blocker that can accept either a regular gastric tube, a suction tube, or a blocker tube.
The study has some limitations. All insertions were performed by an experienced anesthesiologist for patients without airway abnormalities. Sample size is relatively small to achieve accurate evaluation of a certain device such as the SP Blocker to make it widely distributed for routine practice. Moreover, the investigators became unblinded and aware of the used SAD due to the difference in shape between the devices.
CONCLUSIONS
The SP Blocker is a promising device as it offered higher OLP and lower PIP with a greater difference between them, giving a wide safety margin for positive pressure ventilation than the PLMA. The progressive cuff inflation of the SP Blocker limits airway injury. Finally, the SP Blocker could be an acceptable airway device as well as the PLMA so that any anesthesiologist with basic knowledge and without previous training in SADs use could utilize the SP Blocker and solve an important percentage of difficult intubation cases in adults due to its significant hyper-curved, rigid, short, wide airway tube that makes the SP Blocker easy to insert.