
 ENGLISH
ENGLISH




INTRODUCTION
Antimalarial drugs like hydroxychloroquine (HCQ) and chloroquine (CQ) are beneficial in treating rheumatological, dermatological, oncological, and pediatric disorders [1]. However, they can cause irreversible visual loss due to retinal toxicity. Hydroxychloroquine retinal toxicity has a prevalence of 7.5% in patients using the drug for over five years and can exceed 30% with a dose above 5.0 mg/kg after 15 years of treatment [2]. Advanced HCQ toxicity manifests as bilateral bull’s eye maculopathy. Early toxicity shows minimal visual symptoms. Structural macular changes detected through SD-OCT examination are irreversible, and HCQ retinopathy can progress even after stopping HCQ treatment [3]. Detecting the disease at the premaculopathy stage [4] is crucial for regression or limiting disease progression [3]. The objective, non-invasive examination called mfERG can aid in early diagnosis, monitoring disease progression, or assessing recovery after drug cessation [5]. Despite higher sensitivity (92.9%) and specificity (98.1%) compared to recommended tests like automated 10-2 visual fields and SD-OCT [7], mfERG is only discretionary in screening due to limited availability outside clinical centres.
In this study, the authors aim to demonstrate, for the first time in a Polish group of patients, the crucial role of the mfERG test in the early detection of CQ/HCQ pre- maculopathy and emphasize its significance.
MATERIAL AND METHODS
Prospective studies conducted (2015-2020) at 2nd Department of Ophthalmology, Pomeranian Medical Univer- sity, Szczecin, Poland. Patients were recruited from various departments. Data were obtained from 13 asymptomatic patients (15 eyes, mean age: 51 years) treated with CQ/HCQ for over five years, with normal results in routine ophthalmo- logical examination, retinal sensitivity, and macular structure. MfERG results were compared with 13, mean age 51 years, range: 34–66 years, and refractive error matched healthy females (15 eyes). Exclusion criteria: amblyopia, refractive error > ±3.0 diopters, known ocular/systemic diseases affecting retinal function, previous retinal surgery. Informed consent was obtained. Data collected: sex, age, medications, HCQ duration, body weight, daily dose, and systemic disease history (Table I).
Table I
Patients description (n = 13 patients, 15 eyes)
In each patient, the following examinations were performed: routine ophthalmological examination (Snellen distant best corrected visual acuity [DBCVA], refractive error, anterior and posterior segment of the eye, and intraocular pressure [Pascal Tonometer]), retinal sensitivity – AVF 10-2 (W-W), Sita – Humphrey Field Analyzer (HFA; Carl Zeiss Meditec Inc, Dublin, CA) and macular structure – SD-OCT (Cirrus HD OCT Model 5000, Carl Zeiss AG, Jena, Germany) as well as retinal function – mfERG according ISCEV standards [8].
Multifocal Electroretinogram (mfERG) was recorded using the RetiScan (Roland Consult GmbH) system. The protocol of the mfERG test was implemented in the Science version of the system software. Signal recording and analysis were performed in agreement with the First Order Kernel (FOK) technique.
STATISTICAL ANALYSIS
Mean, SD, min, and max values were used for descriptive statistics. Shapiro-Wilk test checked normality assumptions. Comparisons between groups were performed using the U Mann-Whitney test with corrections for small sample sizes when necessary. The sensitivity and specificity of mfERG parameters were calculated. Statistical significance was p ≤ 0.05.
BIOETHICAL STANDARDS
The study was approved by the Ethics Committee of the Pomeranian Medical University in Szczecin (approval No. KB-0012/390/1217).
RESULTS
In a group of 13 females (15 eyes), the mean age was 51 years (range: 35-66 years) (Table I). Most patients had systemic lupus erythematosus (9/13 patients, 69.2%). The mean duration of CQ treatment was 100.5 months (range: 60-204 months) with a mean cumulative dose of 537.9 g (range 195-1,105 g), while for HCQ, the mean duration was 124.8 months (60-204 months) with a mean cumulative dose of 561.6 g (range 260-884 g). In the CQ subgroup, 7 out of 8 patients (87.5%) exceeded the recommended daily dose of 2.3 mg/kg/day for real body weight, whereas in the HCQ subgroup, all five patients exceeded the 5 mg/kg/day limit.
Both the CQ/HCQ group and healthy controls had equal DBCVA (1.0 in both groups), normal IOP (mean 16.4 mmHg, range: 14-18), the normal anterior and posterior segment of the eye, retinal sensitivity (AVF 10-2 [W-W]), and macular structure (SD-OCT; Table II).
Table II
Clinical results of macular structure in patients from the CQ/HCQ group and healthy controls
There was no statistically significant difference in the age between CQ/HCQ group and controls (CQ/HCQ: mean age 51 years, healthy controls mean age: 51 years, U Mann-Whitney test, p = 0.951).
Figure 1 presents the comparison of mfERG parameters (P1 response density, peak time [PT], ring ratio) between the CQ/HCQ group and the control in 6 rings.
Figure 1
Comparison of mfERG parameters in CQ/HCQ group and healthy control groups. Medians (points) and quartiles (whiskers)
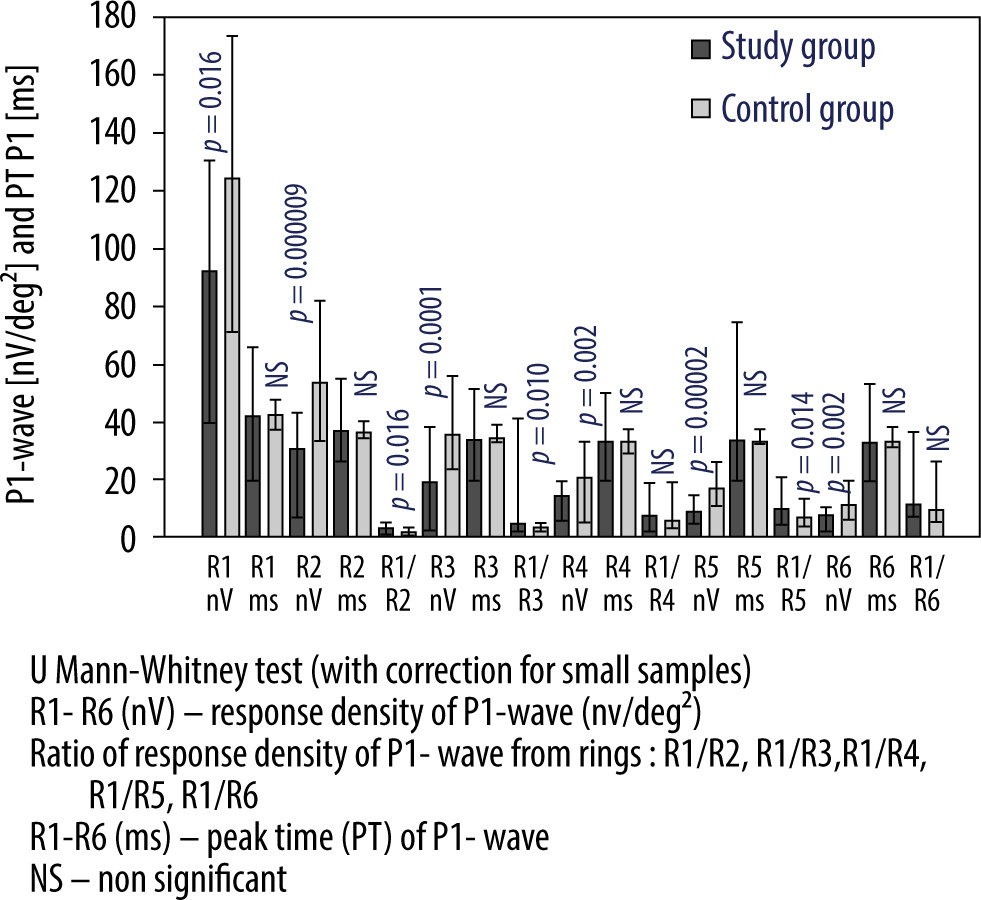
In the mfERG test, in the CQ/HCQ group, the P1-wave response density values in all 6 rings were significantly lower than in the control group (p ≤ 0.016). In addition, ratios of response density of P1-wave were significantly higher than in the control group (except for R4 and R6 ratios). When PT of P1-waves were analyzed, significant differences between CQ/HCQ and control groups were not found (p > 0.35).
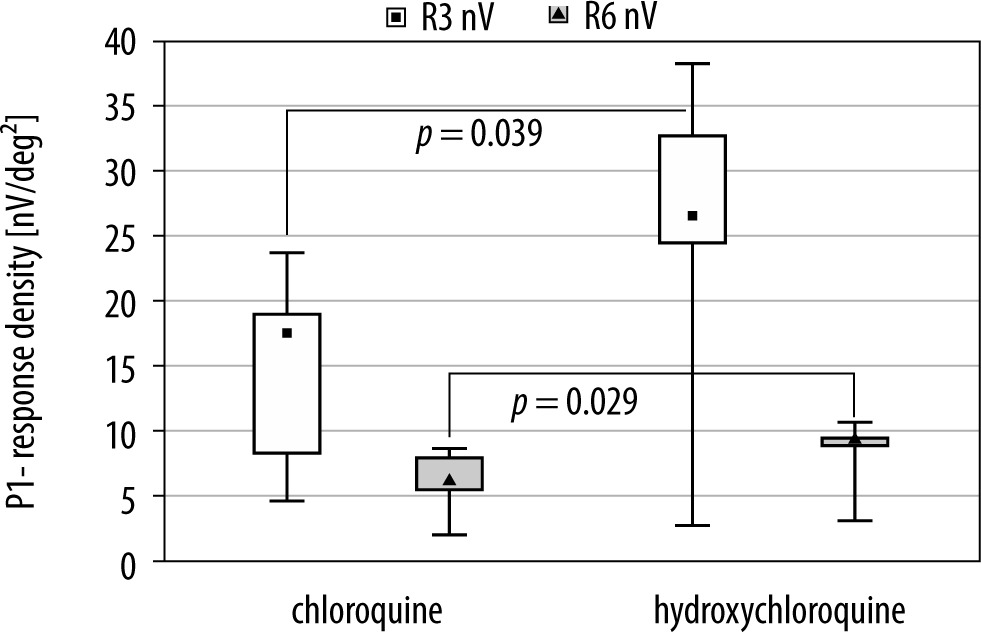
When comparing mfERG parameters among treated patients based on the medication used, the only statistically significant differences were observed in the P1-wave response density values of R3 and R6 (p = 0.039 and p = 0.029, respectively). Patients treated with CQ had significantly lower values in these rings. There were no significant differences in the P1-response density from the remaining rings (p > 0.175; Figure 2).
Figure 2
Comparison of P1-response density from R3 and R6 of mfERG between patients from CQ (n = 9) and HCQ (n = 6) subgroups. Medians – points, quartiles – boxes, minimal and maximal values – whiskers
When comparing the results of P1-wave response density between the CQ subgroup and the control group, a statistically significant reduction was observed in all 6 rings (p < 0.03).
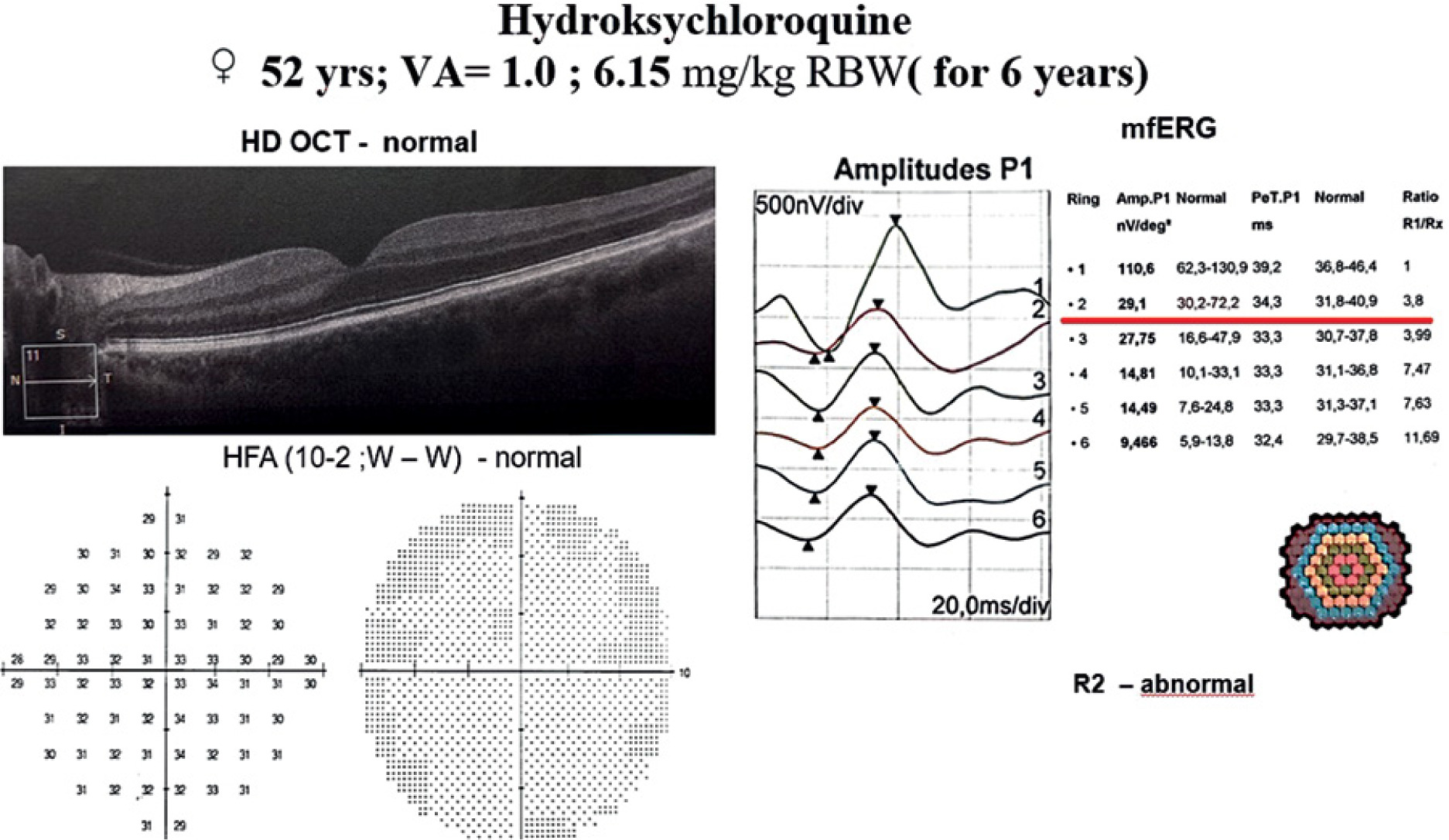
If the results of P1-wave response density from the HCQ subgroup were compared to the control group, a statistically significant reduction was obtained only in R2, R4, and R5 (p ≤ 0.045). A patient case example is illustrated in Figure 3.
ROC analyses were conducted for mfERG parameters for the CQ/HCQ group for six years. High sensitivity and specificity were observed in all rings, with the highest values found in R2 for the P1-wave response density (sensitivity and specificity: 0.93, AUC = 0.98, p < 0.001).
DISCUSSION
The authors conducted for the first time an electrophysiological study based on a Polish group of patients treated with CQ/HCQ for more than five years, using daily doses exceeding safe values. They discovered dysfunction in the cone system, particularly in the macular region, and confirmed the early detection of CQ/HCQ premaculopathy using the mfERG test. Notably, the patients did not experience typical symptoms such as blurred vision, photophobia, scotomas, or reading difficulties [9]. They had very good visual acuity and normal results in complementary examinations. In the entire group receiving CQ and HCQ, there was a significant reduction in P1-wave response density and abnormal ring ratios compared to the control group (p ≤ 0.016; Figure 1). The most pronounced cone system dysfunction was observed in the parafoveal (R2), perifoveal (R3), and mid-peripheral (R5) retina (p < 0.000). Among patients treated with CQ, higher cone dysfunction was detected in rings 3 and 6 (p ≤ 0.039; Figure 2).
When comparing the results of P1-wave response density among the CQ and HCQ subgroups and the control group, in the CQ subgroup, we observed significant retinal dysfunction across all 6 rings (p ≤ 0.003), indicating a widespread retinal dysfunction. On the other hand, in the HCQ subgroup, retinal abnormalities were more localized, primarily affecting only retinal areas in rings R2, R4, and R5 (p ≤ 0.045).
The P1-wave response density had the highest values observed in R2 (sensitivity and specificity: 0.93, AUC = 0.98, p < 0.001), as also reported by Turgut et al. [7].
Chloroquine and HCQ have been known for many years as antimalarial drugs and for their use in the treatment of rheumatoid arthritis and other similar inflammatory diseases. Both CQ and HCQ have a high affinity for melanin. That is why these drugs are concentrated in melanin–rich tissues such as the iris, ciliary body, retinal pigment epithelium and choroid [10]. In humans, it has been shown that CQ is more effective but more toxic than HCQ [9] and demonstrated more frequent ocular side effects. It is the reason why the usage of HCQ is much more frequent and widespread in the world. The most frequent ocular side effect is CQ and HCQ retinopathy which manifest mainly as a “bull’s eye maculopathy” (pigmentary changes in the macula, surrounded by a depigmented zone of retinal pigment epithelium atrophy, which is encircled by a hyperpigmented ring). Although HCQ is less toxic to the retina than CQ, retinal dysfunction occurs and might be detected by the mfERG test. Previously, many authors revealed the value of mfERG in detecting early retinal dysfunction in CQ/HCQ toxicity before the development of visual abnormalities observed in colour vision tests, perimetry, ophthalmoscopy, fluorescein angiography and SD-OCT [11]. Our study’s obtained results agree with those available in the literature and suggest the value of mfERG as a primary screening tool for retinal cone system toxicity in long-term CQ/HCQ treatment.
Additionally, our study was proven to have more severe retinal dysfunction in patients taking CQ, which confirms that CQ is more dangerous for the retina than HCQ. Multifocal ERG demonstrates cone system dysfunction, most commonly in paracentral rings around the fovea [11-13]. This is where the most frequent retinal morphological alterations are detected as a consequence of CQ/HCQ toxicity which can be confirmed in later stages by fundus autofluorescence [14] or SD-OCT [13]. It is also important that functional retinal changes observed in the premaculopathy stage can be reversible, as demonstrated by many authors [11]. Opposite, if retinal structural changes are present and usually detected in SD-OCT (disruption of the parafoveal ellipsoid zone [EZ], parafoveal outer nuclear layer thinning, disruption of the parafoveal interdigitation zone, reduced reflectivity of the parafoveal EZ), the cessation of the HCQ do not stop in majority of cases progression of retinopathy [15]. This is an explanation why patients taking CQ at doses higher than 2.3 mg/kg ABW/day or taking HCQ at doses higher than 5 mg/kg ABW/day or for a long-term duration of more than five years should be considered for periodic mfERG testing for detection of premaculopathy stages of CQ/ HCQ retinopathy.
American Academy of Ophthalmology “Recommenda- tions on Screening for Chloroquine and Hydroxychloroquine Retinopathy” in 2016[6] removed from the essential screening protocol execution of the mFERG test. The main argument for using mfERG in screening protocol only discretionally was a lack of electrophysiological equipment and experienced staff outside clinical centers. We think this is not a sufficient argument based on our results and those available in the literature mentioned above.
LIMITATIONS OF THE STUDY
Our study’s weakness is the small number of cases included in the statistical analysis.
CONCLUSIONS
In conclusion, the results of our study strongly suggest that in patients treated for more than five years with CQ/HCQ, the bioelectrical dysfunction of the cone system was achieved without typical retinal signs of drug toxicity. Multifocal ERG examination revealed significant utility as a screening test to detect premaculopathy stages of CQ/HCQ retinopathy and, in our opinion, should be performed in screening protocol not discretionally but as an essential test.