
 ENGLISH
ENGLISH




INTRODUCTION
Loeys-Dietz syndrome (LDS) is a rare syndrome of genetic birth defects caused by heterozygous mutations in 6 genes (TGFBR1/2, TGFB2/3, SMAD2/3) that encode TGF-ß signaling components. Such heterogeneity indicates high phenotypic variability with considerable diversity regarding the onset time and severity of life-threatening vascular and organ lesions [1, 2]. Loeys-Dietz syndrome is characterized by the presence of vascular lesions in the form of aneurysms and arterial dissections in the central nervous system, thorax, and abdominal cavity, skeletal abnormalities (scoliosis, a sunken chest – pectus excavatum, or a protruding chest – pectus carinatum), dysmorphia, skin changes such as velvety and translucent skin, and easy bruising. Patients with LDS are more likely to suffer from allergic diseases and inflammation of the gastrointestinal tract. Ocular changes have also been documented, including strabismus, myopia, lens subluxation, blue or dark sclerae, and retinal detachment [2, 3].
We aimed to present a case of a child with ocular manifestations of Loeys-Dietz syndrome.
CASE PRESENTATION
A 6-year-old boy was admitted to the Department of Pediatric Ophthalmology, Professor K. Gibiński University Hospital Center, Medical University of Silesia, Katowice, Poland, for ophthalmic diagnosis. He had been diagnosed with LDS; the diagnosis had been confirmed by molecular genetic testing.
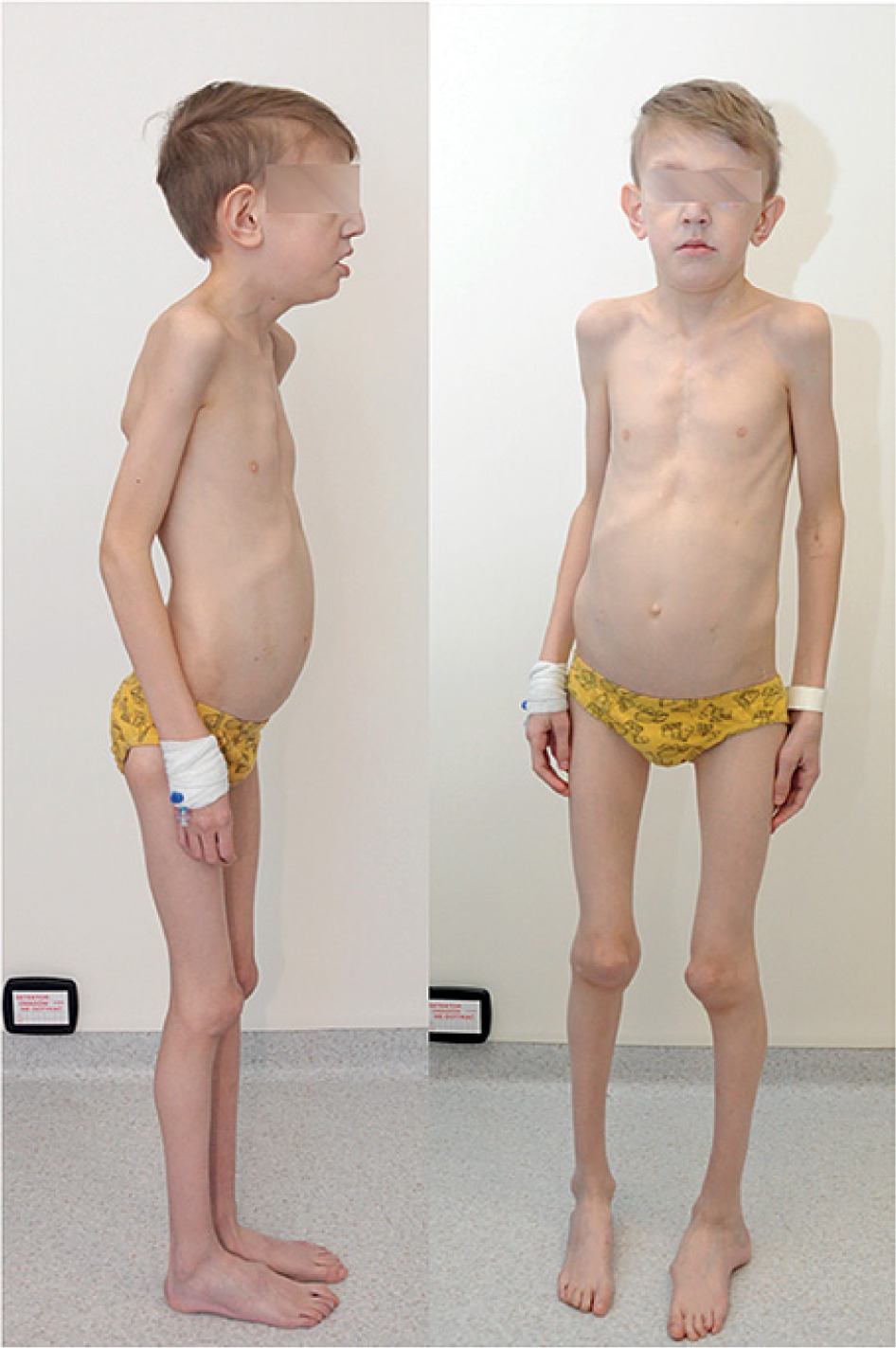
The boy was born at 40 weeks of gestation with a birth weight of 2,900 g and an Apgar score of 9/10. The child is under the regular care of a cardiologist due to chronic heart failure, tricuspid regurgitation, and supraventricular premature beats. In the past, a biological mitral valve was implanted due to a congenital abnormality. The magnetic resonance scans showed dilated fluid spaces in both optic nerve sheaths and a moderate reduction in the optic nerves and optic chiasm volume. Posthypoxic-ischemic lesions were found in the central nervous system. An orthopedist and a physical therapist have supervised the child for osteoarticular changes. The boy has been diagnosed with scoliosis, sunken chest, congenital left foot defect, camptodactyly, and arachnodactyly (Figures 1-3). He also has dysmorphia, hypertelorism, antimongoloid slanting palpebral fissures, deep-set eyeballs, craniosynostosis, submucous cleft palate, and gothic palate (Figures 4, 5).




On the day of admission, best-corrected distance visual acuity was 0.01 in the right eye (correction –19.5 Dsph, –5.0 Dcyl, axis 170°) and 0.3 in the left eye (correction –13.25 Dsph, –1.25 Dcyl, axis 137°). The child could not read any optotypes with the right eye, while the left eye near visual acuity was D –1.5. Visual acuity was checked with a number eye chart. IOP measured with an iCare tonometer was 14 mmHg in the right eye and 15 mmHg in the left eye. A cycloplegic refraction test yielded –22.75 Dsph, –4.5 Dcyl, axis 165° in the right eye, and –18.75 Dsph, –1.25 Dcyl, axis 115° in the left eye. The flash VEP test revealed a 20% delay in P2 latency in the right eye and normal P2 latency in the left eye. The amplitude was at the lower limit of the reference interval for both eyes. The axial lengths were 23.00 mm and 22.05 mm in the right and left eye, respectively.
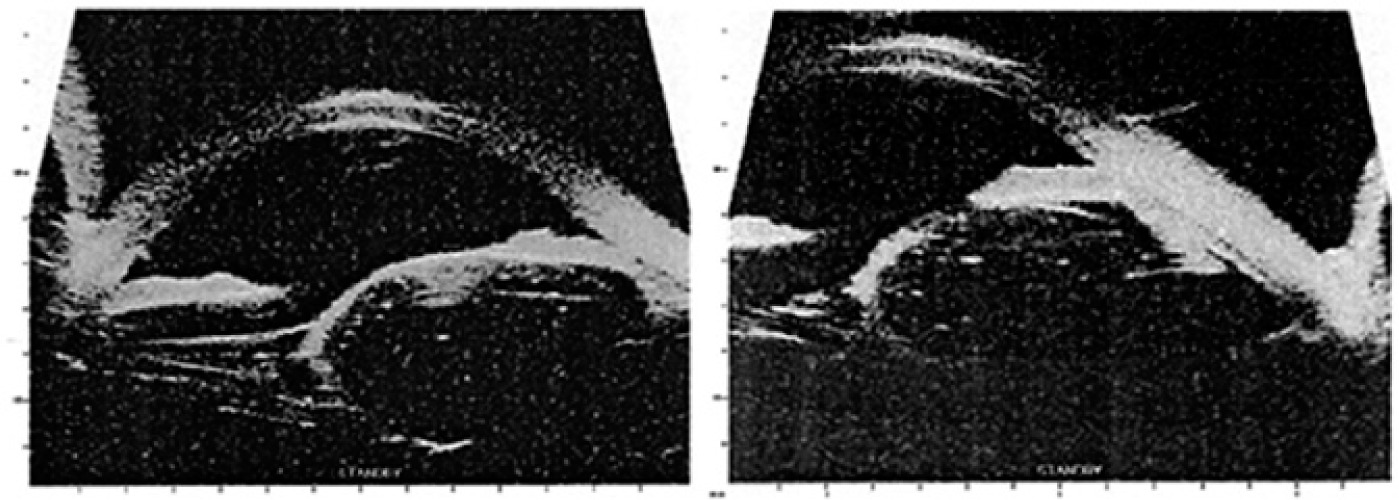
An ocular ultrasonogram revealed a cone-shaped outline of the posterior pole and numerous linear preretinal echoes within the vitreous chamber. Considering superior temporal subluxation of the lenses, UBM was performed, which showed spherical floating lenses with zonular fibres extension and rigidity. The pars plana and ciliary processes were atrophic in both eyes (Figure 6).
After the anesthesiological survey and pediatric consultation, the child was scheduled for surgery to remove subluxated lenses. Due to the child’s general condition, pars plana lensectomy with anterior vitrectomy was performed in both eyes simultaneously. After surgery, levofloxacin, dexamethasone, diclofenac, troxerutin, and mydriatic drops were applied to both eyes. Systemic drugs, i.e., cefuroxime, dexamethasone, and omeprazole, were also administered.
On day five after the procedure, the child was discharged home. The patient’s eye and general condition were good. Parents were instructed to continue the administration of eye drops and systemic medications. Best-corrected distance visual acuity was 0.06 in the right (correction +14.0 Dsph) and 0.3 in the left eye (correction +14.0 Dsph). Best-corrected visual acuity for near was D –3.0 (correction +17.0 Dsph) in the right eye and D –1.5 (correction +17.0 Dsph) in the left eye. Intraocular pressure was 18 mmHg and 14 mmHg in the right and left eye, respectively.
The follow-up ophthalmic examination carried out three months after the surgery showed postoperative aphakia, normal fundus, and no endophthalmitis. Visual acuity improved. BCVA for distance was 0.4 in the right eye (correction +15.5 Dsph) and 0.6 in the left eye (correction +15.5 Dsph). Near vision was D –2.0 (correction +18.0 Dsph) in the right eye and D –1.0 (correction +18.0 Dsph) in the left eye.
Intraocular pressures measured with an iCare tonometer, showing 16 mmHg in both eyes. Ocular ultrasound demonstrated a cone-shaped outline of the fundus, single echoes in the vitreous chamber, and no retinal detachment. The boy’s mother reports he continues progressing well in learning to read and write and enjoys drawing and playing with small blocks. Hence, a significant improvement in the child’s visual function was noted after surgery to remove subluxated lenses.
DISCUSSION
Loeys-Dietz syndrome, a genetically determined rare congenital syndrome, is considered by some authors to be a variant of Marfan syndrome. Ophthalmic changes described in the literature include myopia, blue or grey sclerae, cataracts, retinal detachments, retinal vascular tortuosity, strabismus, and amblyopia [4]. Busch et al. analyzed 25 patients over the age of 16 with genetically confirmed LDS. The patients were followed up for seven years. Ophthalmic examination revealed bilateral ectopia lentis in one patient only. One eye in the study group required surgery due to retinal detachment. No corneal or scleral abnormalities or retinal vascular tortuosity were found in any of the study eyes [3]. Since LDS shares some clinical features with Marfan syndrome, where the incidence of lens ectopy ranges from 30.2% to 50.7%, genetic testing should be performed; lens subluxation in LDS is not common [5, 6]. In the case we analyzed, lens subluxation was present in both eyes and was clinically significant, causing difficulties with near and far visual function due to lens floating with the child’s eye and head movements. Ultrasound biomicroscopy confirmed a considerable degree of lens subluxation, which, combined with the child’s high level of physical activity and the need for rehabilitation, posed a threat of lens dislocation into the vitreous chamber. Considering this, and after obtaining the informed consent of the legal guardians, we decided to perform lensectomy in both eyes. Like Busch et al. [3], we found no retinal detachment or tortuosity of the retinal vessels. We also found no abnormalities in the structure of the cornea and sclera. Our literature review on LDS showed that lens subluxations requiring surgery are extremely rare. One of these few reports is a paper by Braverman et al. on a 44-year-old woman with bilateral lens subluxation. However, the authors emphasized that this was LDS type 4, where subluxation occurs in middle age [7].
Due to his ophthalmic condition, the child was again referred to the Genetic Clinic for thorough genetic testing and differentiation with Marfan syndrome.
CONCLUSIONS
Children with genetically determined congenital syndromes should be constantly monitored by an ophthalmologist for a thorough evaluation of the eyes and a prognosis of the development of visual function.
In case of ocular changes atypical of the syndrome diagnosed by the geneticist, the ophthalmologist may order repeat genetic tests to verify the original diagnosis.