




Parathyroidectomy (PTX) is the treatment of choice, with a cure rate of 95–98% in expert centres [1, 2]. Commonly inadequate resection is caused by ectopic glands. Mostly they are found in the superior mediastinum among the thymus gland and can be excised by a collar incision [3].
A mediastinal parathyroid (MP) is determined as a gland found completely below the level of the clavicle. Approximately 15–20% of abnormal parathyroid glands are found in the mediastinum. Ectopic inferior parathyroids are frequently located in the anterior mediastinum, usually in the thymus gland, while superior parathyroids are found in the posterosuperior mediastinum. Less commonly they may be located in the aortopulmonary window and rarely in the pericardium [4–6].
We report 4 patients operated by upper median sternotomy for primary hyperparathyroidism (PHP) due to ectopic mediastinal lesions.
Between the years 1983 and 2018 a total of 1019 patients underwent surgery for PHP at our institution. Among this group of patients 66 (6.5%) were operated for ectopic lesions localized in the mediastinum. In 62 (94%) patients the ectopic lesions were excised via cervicotomy, 4 of whom required an upper median sternotomy approach. There were 2 women and 2 men, aged 22–72, mean 52.5 years. The diagnostic and surgical approaches used for our 4 patients are shown in Table I.
Table I
The diagnostic and surgical approaches
All patients diagnosed for PHP were referred to our department for further treatment, from other centres. Apart from one woman admitted for threatened hypercalcaemic crisis (1.63 mmol/l), the reminder had scintigraphy Tc99-MIBI/SPECT performed.
Patient 1: This was a 72-year-old woman who complained of general weakness, consciousness disorders, and bone pain. A ultrasonography (USG) of the neck revealed multinodular thyroid gland and probably enlarged left upper parathyroid gland (11 × 7 mm). During the operation both upper parathyroid glands were removed. No lower parathyroid gland was seen and ionized parathormone level (iPTH) did not decrease; near total thyroidectomy was performed. After the operation her condition worsened and on the 7th postoperative day helical computed tomography (CT) scanning was performed. The examination revealed a mass 30 × 20 × 20 mm in the aorto-pulmonary window. Moreover, pathologic fracture Th8-Th9 was seen. She was re-operated the next day, and the lesion was excised. The post-operative period was complicated with bilateral pneumonia and serious hypocalcaemia. On day 27, after the second operation, the woman was discharged to her previous hospital in a good condition, where she spent next 16 days with a recommendation to take calcium. She survived 7 years under oncological supervision, until in August 2016 she was lost from observation.
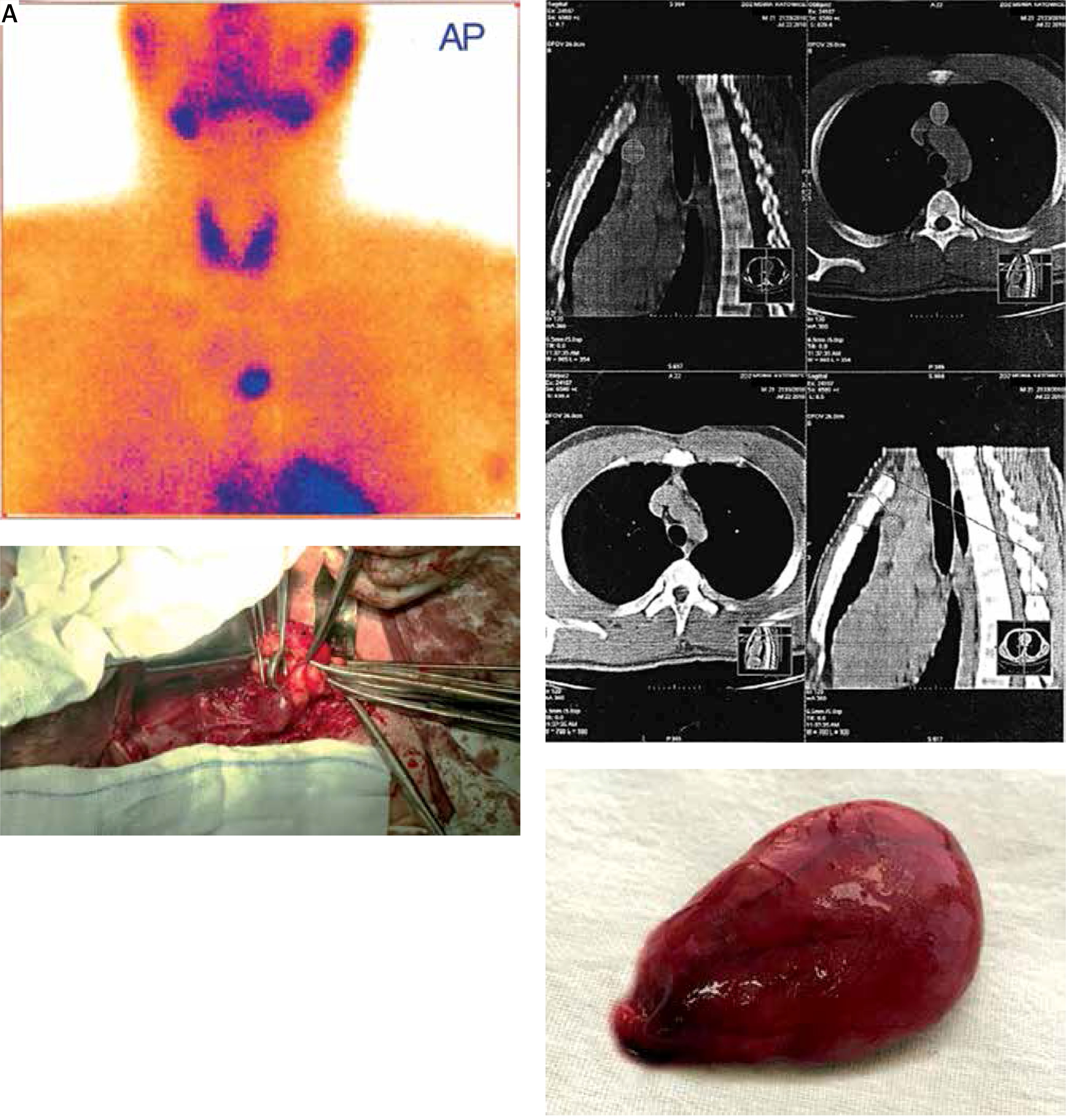
Patient 2: This was a 22-year-old man treated without success for a renal stones and renal insufficiency. During treatment it was noticed that his serum ionized calcium level (iCa) had risen (2.13 mmol/l), creatinine was elevated to 2.46 mg/dl, and glomeruralar filtration rate (GFR) dropped to 35 ml/min/1.73 m2. Scintigraphy with Tc99m-sestamibi showed an extrathyroidal accumulation area projected onto the superior mediastinum located slightly left of the median line (Figure 1 A). A one-stage operation (cervicotomy and middle superior sternotomy) was carried out, with positive biochemical effect. A parathyroid lesion 20 × 21 × 25 mm was found hidden inside the left lower thymus horn and surrounded by the pleura. On the first post-operative day he complained of abdominal pain, partly in the upper abdominal area, radiating to the back with nausea and abdominal distention. The physical examination findings revealed mild tenderness of the whole abdomen and distention. Serum amylase level increased to 756.6 IU/l, glucose 165 mg%, serum lactate dehydrogenase (LDH) 365 IU/l, C-reactive protein (CRP) 178.6, creatinine 3.6 mg/dl, white blood cells (WBC) 17,200 cells/mm3, aspartate transferase (AST) 275 U/100 ml, and bilirubin 3.6 mg%. CT examination showed grade C according to the Balthazar-Ranson grading system. They returned to normal on the 14th postoperative day. The patient recovered and was discharged on the 22nd post-operative day. USG and CT examinations performed before he left the hospital revealed pancreatic pseudocyst. He is currently alive. A control CT scan showed that the pseudocyst has diminished.
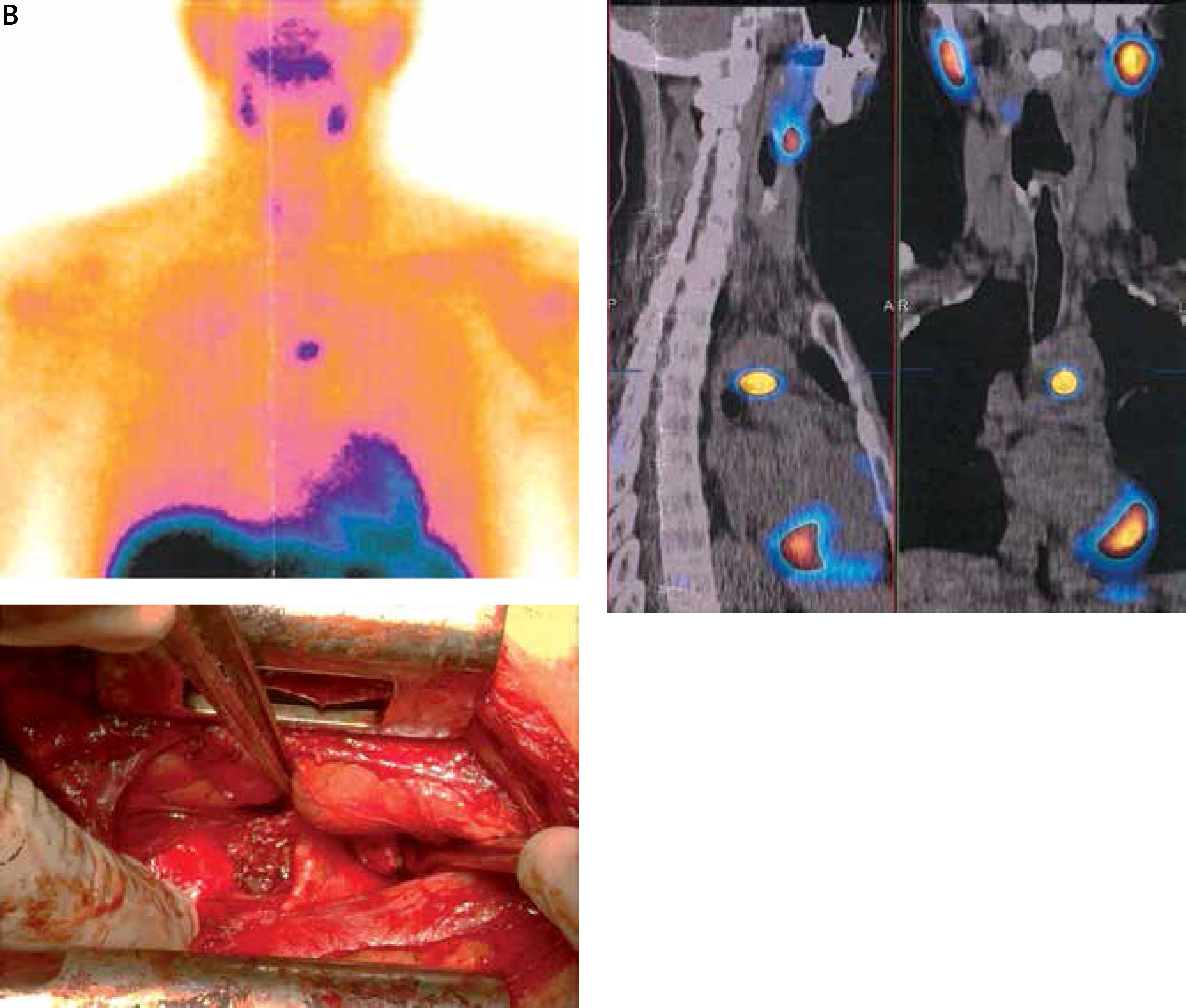
Patient 3: This was a 54-year-old woman diagnosed during laboratory screening. She complained of renal stones and hypertension. A sestamibi scan revealed a single focus of increased tracer accumulation in the anterior mediastinum. Unfortunately, before operation, the patient refused sternal approach, following failed cervicotomy, and allowed only the collar incision. After the cervicotomy, she once again refused the sternal approach. However, after 16 months she gave permission for sternotomy. The main complaints, such as bone pain, weakness, and walking troubles, increased. The upper middle sternotomy was done. A parathyroid lesion 10 × 15 × 20 mm was found hidden very deep between the main left bronchus posteriorly, the left pulmonary artery anteriorly, and 2 cm below the aortic arch, close to the aorta (Figure 1 B). She is currently alive, under supervision, and in good condition.
Figure 1. B
Parathyroid hyperplasia located in the mediastinum. CT and scitigraphy images (female age 54)
Patient 4: A PHP was diagnosed during a routine laboratory screening in a 62-year-old man for complaints such as weakness, fatigue, and bone pain. A sestamibi examination demonstrated a single focus of increased tracer accumulation of the anterior mediastinum. During a 1-stage operation (cervicotomy and middle superior sternotomy) a huge lesion 50 × 40 × 30 mm was excised. It was found in the angle of the caval superior and the left brachiocephalic veins anteriorly and the aortic arch posteriorly. The patient recovered and was discharged on the 8th post-operative day. He remains under supervision.
Mediastinal location is the most likely when the parathyroid gland has an ectopic position [3, 7]. Meta-analysis of a group of 7529 patients showed that 15.9% of parathyroid glands were present in ectopic locations, with more than 4% within the mediastinum [4]. Most ectopic mediastinal parathyroid glands are located in the thymus, or more often in the cervical tongue of the thymus in the anterosuperior mediastinum. Such lesions can be mostly removed through standard cervical approach; however, those located deeper require sternotomy. Others [3, 8] reported that in 1–2% of patients treated for PHP, sternotomy was necessary when parathyroid glands were located in the middle or posterior mediastinum, aortopulmonary window, or pericardium. Another reported that if the mediastinal parathyroid gland was located below the innominate vein, an open thoracic approach should be used [9].
Parathyroid changes found deep in the mediastinum remain a surgical challenge. For these lesions preoperative localization is crucial before mediastinal exploration. However, the optimal approach has not been determined. Unlike parathyroid changes in the neck, USG has not been proven useful in detecting mediastinal parathyroids. In such ectopic glands CT scan or magnetic resonance (MR) may be helpful. Single photon emission tomography (PET) can also improve localization, with up to 96% sensitivity [8, 10]. For imaging of parathyroid lesions Tc99m-sestamibi has a very important benefit: it allows identification of smaller lesions than former examinations. So, the SPECT/CT remains the best imaging modality for preoperative localization of parathyroid lesions. If ectopic changes are suspected, addition of 4D-CT is recommended. Actually, preoperative FCH PET/CT has a high value for parathyroid lesions detections in patients with PHP [11, 12].
Some authors suggested the level of the aortic arch on the horizontal chest CT as a guideline for suitable surgical approach during PTX [13]. Another demonstrated that when the parathyroid lesion was located deeper than 6 cm below the clavicle head, a transcervical approach was effective only in 25% of cases [14]. All changes above the aortic arch in the antero-superior mediastinum can be treated successfully by transcervical approach, while those in the middle or posterior mediastinum can be cured by transthoracic approach [15]. On the other hand, 1–2% of patients will require a transsternal or transthoracic approach due to deeply seated mediastinal lesions [16]. Our series confirmed that only a small number of patients require a direct sternal or thoracic approach, in accordance with other findings.
However, complete resection via a cervical approach might be difficult or impossible when the lesions are located in the lower part of the mediastinum below the innominate vein. The deep location in the middle mediastinum is the main risk condition for unsuccessful cervical approach. We agree with such observations [13, 15, 16]. Our series confirmed such findings that few patients require a direct sternal or thoracic approach. To reduce the invasiveness of full sternotomy we prefer upper middle sternotomy, which was done in 4 of our patients [17]. Three out of 4 of our patients had cervicotomy performed. Unfortunately, we did not find any parathyroid glands, and superior middle superior sternotomy was necessary. During such a procedure we cut the sternum for 5–7 cm only. This approach allowed us an excellent view of the middle mediastinum, particularly into the aorto-pulmonary window. Nevertheless, despite a higher risk of complications, sternotomy seems to be safe procedure. Among our patients we observed 2 incidences of one-sided pneumothorax and 1 incidence of pneumonia. After pleural cavity drainage, chest tubes were removed on the 3rd postoperative day.
Some authors [3, 15, 18] advocate a median complete sternotomy. They consider that only such drastic action gives a good view and makes it easy to palpate any other masses that are present in the mediastinal fat. Another advocates also anterior mediastinotomy (parasternal) with an 89% success rate, or thoracotomy [19]. In the last 2 decades less invasive approaches have been introduced, following new imaging techniques to identify ectopic lesions. Such procedures as video- and video-assisted thoracoscopy or robotic surgery reduce the rate of morbidity, shorten the stay in hospital, and significantly decrease pain, but palpation sensitivity is limited [20–22]. Moreover, unfortunately most thoracoscopic procedures are not accessible in endocrinal surgical centres. On the other hand, a review of thoracic centre reports shows up to 23% of failed operations for mediastinal location of the parathyroid glands [3, 15].
Upper middle sternotomy is still a good access in the search for ectopic parathyroid glands in the mediastinum.