









Introduction
The optimum age for the female reproductive ability is 18-30 years, after which there is gradual decline in the reproductive ability and ovarian function [1]. Ovarian surgery has negative impact on the ovarian reserve and reproductive ability [1].
Somigliana et al. studied the ovarian response to controlled ovarian hyperstimulation (COH) during in-vitro fertilization (IVF) in women who had an excision of endometrioma in the past [2]. Somigliana et al. found significant difference in the number of oocytes retrieved in the operated ovary compared to the non-operated ovary irrespective the size of endometriomas [2]. Yılmaz et al. found that the surgical excision of endometrioma associated with decreased ovarian reserve (DOR) [3].
The effect of surgical excision of endometrioma on the ovarian reserve is extensively studied and it is difficult to conclude whether the DOR after surgical excision of endometrioma is because of surgery alone and/or due to microscopic implants of endometriosis within the ovarian stroma around the excised endometrioma [1]. In addition, the studies regarding the effect of surgical removal of benign ovarian lesions other than endometriomas on the ovarian reserve are limited. Therefore, this report represents finding of reversible decreased ovarian reserve (RDOR) after conservative ovarian surgery for benign lesion other than endometrioma.
Case report
A 36-year-old woman presented with abdominal pain and diagnosed provisionally as complicated ovarian cyst. The trans-vaginal ultrasound (TVS) done for the studied woman showed, well-defined solid mass, measuring 10 × 8 cm related to the anterior uterine wall most probably subserous uterine leiomyoma or ovarian fibroma. The TVS finding of left solid mass was confirmed by the magnetic resonance imaging (MRI).
The studied woman signed written consent, agreed for exploratory laparotomy after departmental approval. At laparotomy, the solid mass was originating from the left ovary and the right ovary and uterus were completely normal. The left ovarian mass excised [4] (Fig. 1), and more than half of the left ovary was preserved during surgery for future fertility.

The pre-operative ovarian reserve hormones, anti-Müllerian hormone (AMH 2.3 ng/ml), follicle stimulating hormone (FSH 3.5 mIU/ml), and luteinizing hormone (LH 3.0 mIU/ml) were completely normal. The microscopic examination of the excised mass showed bundles of spindle cells without mitotic activity, confirming the diagnosis of ovarian fibroma.
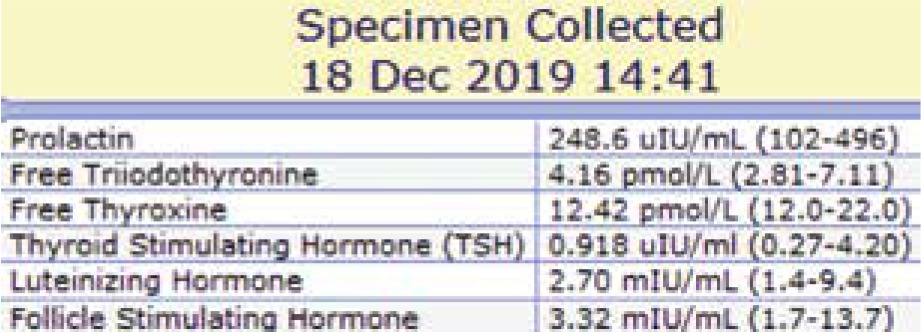
Post-operative follow-up of the studied woman for one year showed; regular menstrual rhythm, duration, elevated FSH (Fig. 2) and LH (Fig. 3) and both the FSH and LH returned to normal levels at the end of the first post-operative year. Patient`s body weight, body mass index (BMI), AMH, prolactin and thyroid profile (Fig. 4) did not show any changes during the post-operative follow-up.


Fig. 4
Follicle stimulating hormone (FSH), luteinizing hormone (LH), prolactin and thyroid profiles at the end of the first post- -operative year of follow-up
This report represents finding of RDOR after conservative ovarian surgery for benign lesion other than endometrioma to minimise normal ovarian tissue damage during surgery as much as possible and to counsel women at risk of DOR that any ovarian surgery may be associated with further decrease in the ovarian reserve and reproductive ability.
Finding of RDOR after conservative ovarian surgery for benign lesion other than endometrioma included: 1) elevated both FSH and LH (both the FSH and LH returned to normal levels within 1-2 years post-operative); 2) regular menstrual rhythm and duration; 3) no change in the body weight and/or BMI; 4) normal AMH, prolactin and thyroid profile.
Discussion
Ovarian reserve reflects the number of the oocytes available in the ovaries of any woman and her reproductive ability [5]. Women at increased risk of DOR include: 1) > 35 years old; 2) family history of premature ovarian failure; 3) past history of ovarian surgery and/or radiation; 4) unexplained infertility [6, 7]. In addition ; Balmagambetova et al. concluded that exposure to environmental hazards may destroy a considerable number of the ovarian follicles with subsequent DOR [8].
National Institute for Health and Care Excellence (NICE) guidelines concluded that sufficient ovarian reserve diagnosed by either antral follicle count (AFC) > 4 or serum AMH level > 5.4 pmol/l or serum FSH level < 8.9 IU/I [9].
The studied woman was at risk of DOR because of her age (over 35 years) [6, 7] and because of ovarian surgery. She was worried about her fertility and reproductive ability; therefore, the hormonal profile done for her every month during the first 3 post-operative months, then every 3-4 months during the first post-operative year.
Post-operative follow-up of the studied woman for one-year showed; regular menstrual rhythm, duration, elevated FSH and LH for one year after surgery (both the FSH and LH returned to normal levels at the end of the first post-operative year). Patient’s body weight, BMI, AMH, prolactin and thyroid profile did not show any changes during the post-operative follow-up.
The finding of RDOR after conservative ovarian surgery lesion other than endometrioma included: 1) elevated both FSH and LH (both the FSH and LH returned to normal levels within 1-2 years post-operative; 2) regular menstrual rhythm and duration; 3) no change in the body weight and/or BMI; 4) Normal AMH, prolactin and thyroid profile. The studied woman was at risk of DOR and she developed RDOR for one year after surgery according to the NICE guidelines which diagnosed sufficient ovarian reserve by serum FSH level < 8.9 IU/I [9].
Although, Yılmaz et al. concluded that the bipolar diathermy used during surgical excision of endometrioma is the most harmful hemostatic modality to ovarian reserve [3] and Deckers et al. systematic review concluded that the bipolar electrocoagulation negatively impacts ovarian reserve, especially for women with reproductive goals [10].
Owczarek et al. studied the effect of the hemostasis techniques on ovarian reserve following laparoscopic enucleation of endometriotic cysts and concluded that the laparoscopic enucleation of endometriotic cysts leads to DOR, regardless the hemostasis technique used [11].
Recently, Younis et al. systematic review concluded that endometrioma cystectomy (especially bilateral), associated with DOR and may have no obvious reproductive advantage, therefore, conservative treatment should be considered as the first line of treatment [12]. Indeed, it’s not clear whether the DOR after endometrioma excision is because of surgery alone and/or due to microscopic implants of endometriosis within the ovarian stroma around the excised endometrioma [1].
During the surgical excision of the left ovarian fibroma of the studied woman, the surgeons did not use any electrocoagulation hemostatic modality (only surgical stitches used), half of the left ovary was preserved, and the right ovary was completely normal. Despite of the above-mentioned conservative measures, the studied woman developed RDOR for the first post-operative year.
The effect of surgical excision of endometrioma on the ovarian reserve is extensively studied, while, the studies regarding the effect of surgical removal of benign ovarian lesions other than endometriomas on the ovarian reserve are limited.
To the best of our knowledge, this report is the first report represents the finding of RDOR after conservative surgery for benign lesion other than endometrioma and large studies are needed to confirm the authors' finding.
Conclusions
This report represents the finding of RDOR after conservative ovarian surgery for benign lesion other than endometrioma to minimise normal ovarian tissue damage during surgery as much as possible and to counsel women at risk of DOR that any ovarian surgery may be associated with further decrease in the ovarian reserve and reproductive ability.