

Introduction
Measles is a highly contagious viral disease that causes a high-rate of morbidity and mortality. Effective vaccination with measles-mumps-rubella (MMR) vaccine made this disease easily preventable. Despite widespread accessibility to the vaccine and obligatory vaccination with MMR at the age of 12-13 months and again at 6-10 years of age (depending on the country), anti-vaccine movements have contributed to a decrease in vaccine coverage. Efficient herd immunity can be obtained when the vaccine coverage exceeds 95% [1-3]. Data from the National Institute of Public Health – National Institute of Hygiene (NIPH-NIH) indicate an increasing ratio of diagnosed measles; the number of measles cases in 2018 was 5-times higher than that in 2017 (339 vs. 63) [4]. Measles outbreaks are now occurring all around the world as a response to decreased herd immunity. According to the European Centre for Disease Prevention and Control (ECDC), vaccination coverage is below 95% in most European countries, and the highest number of confirmed cases were reported in France, Italy, Bulgaria, Lithuania, and Poland, with more than 100 cases in April of 2019 [5].
In 2010, the World Health Organization, Office for Europe, undertook a resolution signed by all countries in the WHO European region, to eliminate measles and achieve sufficient herd immunity [6]. Unfortunately, in Poland the ratio of vaccination, which should have increased, continues to decrease with a ratio below 93% in 2018 [4].
Measles virus infection causes life-long protective immunity, while two doses of MMR vaccine should also provide appropriate immunization [3]. However, there are some reports suggesting that the immune response to measles following MMR vaccination provides less-sufficient immunization and that the amount of specific anti-measles immune antibodies (IgG class) decreases over time [7, 8].
The aim of this study was to analyze the seroprevalence of anti-measles IgG antibodies among patients referred for testing in a central laboratory of the Central Teaching Hospital of University Clinical Centre in Warsaw, Poland.
Material and methods
Analyzed data
The study was conducted from March to June of 2019. Retrospective analysis included results for measles-specific IgG from 364 tested patients. The age of enrolled subjects ranged from four months to 101 years, with a median age of 46 and a mean age (SD) of 43 ±18. There were a total of 245 women and 118 men tested. Adult patients, who were tested with regard to measles-specific IgG, were either health care workers or patients who were suspected of having contact with active measles virus within the last 48 hours. All analyzed data were anonymized; the basis of study was age, sex of patient, and the reactivity of anti-measles IgG measured using commercial Liaison® indirect chemiluminescence immunoassay on the DiaSorin Liaison® automated analyzer, which has been proven highly specific and sensitive in the detection of measles-specific IgG [9]. The threshold value regarded as protective immune status was 16.5 AU/ml [border line 13.5-16.5 AU/ml; lower limit of detection (LoD) at 5 AU/ml and higher LoD at 300 AU/ml]. Study was accordant with the regulation of Bioethics Committee of Medical University of Warsaw.
Statistical analysis
Data analysis was performed using GraphPad Prism v.6 (GraphPad Software, La Jolla, CA, USA). The type of data distribution was analyzed using the D’Agostino-Pearson omnibus normality test. The seroprevalence was analyzed using the modified Wald method. Differences between studied groups were evaluated using the Kruskal-Wallis test. The Mann-Whitney test was used to compare the serological status between men and women. The χ2 or Fischer exact tests were used to compare the seropositivity rates between different groups. A p-value less than 0.05 was considered statistically significant.
Results
Total number of 284 patients had measles-specific IgG antibodies concentrations higher than 16.5 AU/ml, thus the seropositivity was 78.02% (95% CI: 73.48-81.98). The study group was divided into seven age groups, based on their possible MMR vaccination: 1) 0-1 years old (n = 13, before obligatory vaccination at age 13-14 month); 2) 1.3-16 years old (n = 17, children who should be vaccinated with two doses of MMR vaccine); 3) 19-38 years old (n = 88, young adults who should be vaccinated with two doses of MMR vaccine); 4) 39-45 years old (n = 61, adults who should be vaccinated with one dose of MMR vaccine); 5) 46-59 years old (n = 131, adults who were not covered by an obligatory vaccination programme, occupationally active); 6) 60-69 years old (n = 36, adults who were not covered by an obligatory vaccination programme, partially occupationally active); 7) 70-101 years old (n = 16, adults who were not covered by an obligatory vaccination programme, retired). In the group of adult subjects, the percentage of seropositivity was estimated at 80.12% (95% CI: 75.48-84.07). The distribution of anti-measles IgG in each age group is presented in Table 1.
Table 1
Characteristic of studied groups with exact results of measles-specific IgG prevalence and values
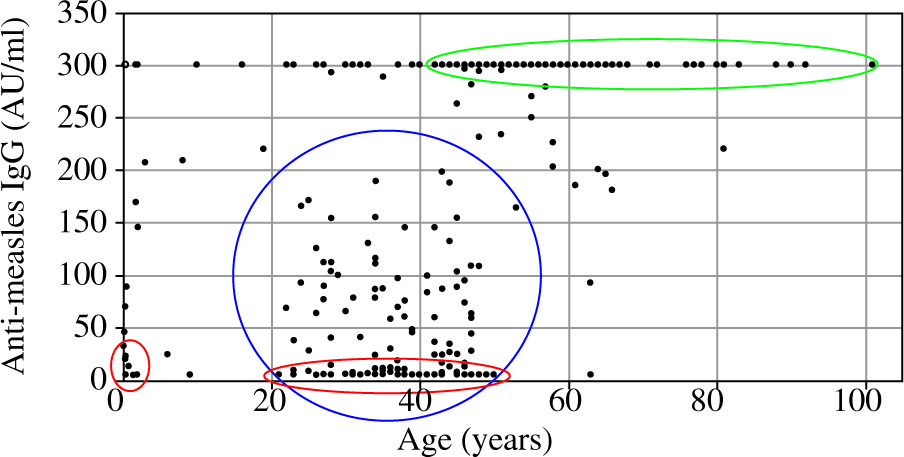
There was a significant difference in anti-measles IgG concentration between men and women, indicating that men have a lower level of specific anti-measles antibodies (median values 145.5 vs. 300 AU/ml, p = 0.033). An age dependence of antibody concentrations was observed (Fig. 1) and divided into three groups based on distribution: two with the lowest and one with the highest concentration of antibodies. The first group included patients with the lowest values in the 0-1 years old group. The second group included 20-45 years old patients, and the third group included patients older than 45 years, in which anti-measles IgG concentrations reached the highest values (Fig. 1). Individuals aged 20-45 had the most diversified distribution of results.
Fig. 1
Distribution of IgG anti-measles antibodies according to patient’s age. Red circles show the population with seronegativity, the green circle shows the group with the highest level of immunization, and the blue group showed the highest diversity
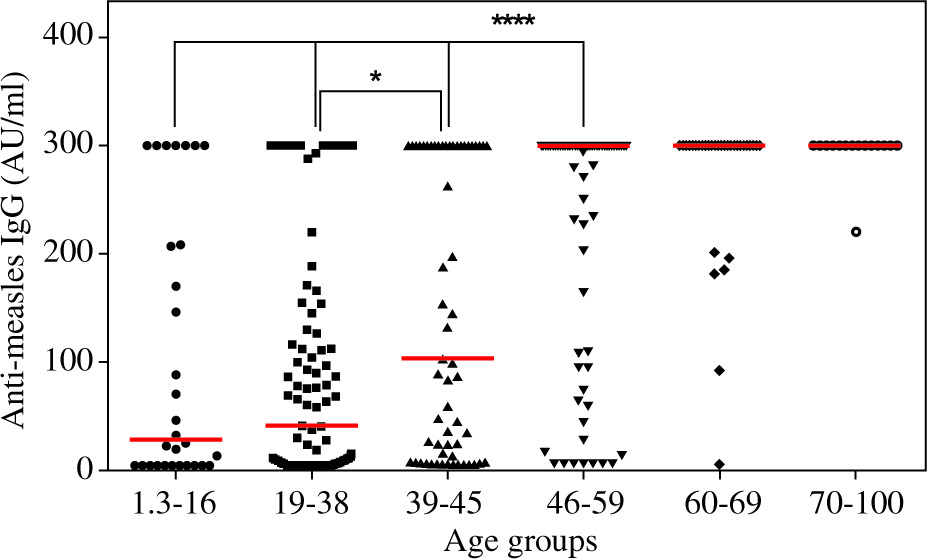
A significantly higher number of seronegative patients were in the male group than in the women group (p = 0.04). The studied groups differed significantly in measles-specific IgG values, which are presented in Table 1 and Figure 2. There was also a significant difference in the seronegativity/seropositivity ratio between examined aged groups, with the lowest seropositivity ratio in the group of subjects that were 19-38 years old (Fig. 3).

Discussion
The results showed that 78.02% of patients enrolled in the study had positive titres of measles-specific IgG antibodies. The lowest ratio of seropositivity was found in a group of adult patients who were covered by an immunization schedule with two doses of MMR vaccination in childhood, and in a group of children aged 0-1 who were not covered by vaccination. This observation is consistent with the results from other studies [10]. According to the immunization schedule appropriate for each study group, a second vaccination should have been administered at the age of 7-10, which means that the time between the last vaccination and the test for the presence of specific IgG was 9-28 years. Interestingly, the seropositivity ratio was higher in a group that, according to immunization schedule, should have administered one dose of MMR; however, we cannot exclude that this group also involved non-vaccinated subjects, since coverage of vaccination in 1978 was estimated at 50% and in 1981 it was ~80% [11]. The seropositivity ratios observed in our study between vaccinated once and twice are not accordant with the results from a study performed in Japan [12]. Here, we show a significantly lower titer of antibodies in the group vaccinated twice than after one dose of MMR. In addition, the seropositivity ratio was the highest in all groups, which were not vaccinated due to natural immunization caused by the disease. Nevertheless, the number of seropositive subjects was quite low compared with that of other European studies [2, 3, 13], which does not confirm that immunogenicity from the measles vaccine has life-long effects [14]. We observed that a group of patients who were covered by immunization schedule had significantly lower titres of antibodies against measles that a non-vaccinated older group, which is consistent with the results from previous studies [3, 8, 13, 15]. Also, our results showed a similar distribution of anti-measles IgG among different age groups as shown by Ristic et al. [13]. Here, we observed the same trend of decreasing measles-specific IgG titer over time from vaccination, as reported by Kennedy et al. [7]; however, there was a longer time between possible vaccination and serological test in our study (up to 40 vs. 17 years). Our results are consistent with those obtained by Coppeta et al. who showed that total seropositivity reached 87% in a group of adult hospital employees, with the highest ratio in a group of patients not vaccinated in childhood (born before 1982) and lowest in the group born in 1992-1999 [1]. In contrast to previous studies, our results showed a statistically significant difference in seropositivity ratios between men and women [1-3, 10, 16, 17]. Higher immunization status in women might be associated with additional vaccination against rubella, which was administered together with vaccine against mumps and measles later in childhood. We observed an alarming susceptibility to disease in 56/149 (37.58%) individuals who were 19-45 years old, and this rate is almost twice that reported in other studies [3, 13, 18] and similar to the results reported in studies conducted in South Korea, Italy, and Czech Republic [14, 15, 19]. These data strongly suggest that this age group is at particular risk of possible infection and should be re-vaccinated. This includes health care workers, teachers, or others who work with people who might be a reservoir of the virus. However, as it was suggested by the Italian National Plan for Measles and Congenital Rubella Elimination, foreign-born women who are registered for the first time in the Italian healthcare system, should be additionally vaccinated [18].
Conclusions
The main limitation of this study is a lack of information about vaccination status among enrolled subjects. Given the retrospective nature of this study and patients’ personal data anonymized, we were not able to obtain such medical records. Despite this limitation, our results are reliable and consistent with those of other national [11] and European studies. These results warrant further discussion about modification of immunization schedules with regard to recommended vaccines in adulthood. Such a suggestion concerning vaccination against mumps, which is administered with the MMR vaccine, has already been raised [20]. From an economical point of view, it should be considered if preventive vaccination is more cost-effective than previous screening of specific anti-measles IgG antibodies in the most susceptible groups. Studies performed on mumps immunization strategy in Italy showed that screening for antibodies and re-vaccination of individuals who were seronegative only is less expensive than vaccination without confirmation of serological status [21]. An appropriate analysis should be performed with regard to measles immunization, given that the seropositivity ratio in young adults is not sufficient to retain expected herd immunity level.