







Rupture is the most frequent complication of abdominal aortic aneurysm (AAA) and is fatal in as many as 60–80% of patients [1]. The risk of rupture increases with the aneurysm size, expansion rate, continued smoking, persistent hypertension, and when symptoms occur [2]. Thus, a large and symptomatic AAA due to high risk of rupture requires an urgent repair. Endovascular aneurysm repair (EVAR), though less invasive than an open surgical repair, may still be contraindicated in some high-risk patients [3]. In this report a successful treatment of a patient with a severe aortic stenosis and a symptomatic, large abdominal aortic aneurysm with a simultaneous balloon aortic valvuloplasty (BAV) and EVAR is presented.
An 87-year-old female was referred to a vascular surgery department because of a symptomatic AAA. She reported abdominal pain and also had a recent history of gastrointestinal bleeding. She also presented weakness, dyspnoea on exertion, and poor tolerance of physical exercise; she had to stop after climbing 2 flights of stairs. She suffered from arterial hypertension and was on losartan, hydrochlorothiazide, and acetylsalicylic acid.
On physical examination she was conscious and afebrile. On auscultation breath sounds were generally normal with some fine crackles at the base of the lungs, heart rate was regular, 80 beats per minute, and a loud systolic murmur was audible. Her blood pressure was 138/80 mm Hg. The abdomen was soft, with a slightly tender on palpation, pulsatile mass in the mid-abdomen. On admission she was anaemic (HGB 8.5 g/dl) and had a moderate chronic kidney disease (serum creatinine 1.12 mg/dl and GFR (MDRD) 48.9 ml/min/1.73 m2). ECG showed sinus rhythm, regular 70/min, QS in III, aVF, poor R-wave progression in V1-V3, and single supraventricular ectopy. The vascular POSSUM scores were as follows: physiology score 30 and operative severity score 14. Risk of morbidity was 82.5%, and risk of mortality was 15.8%.
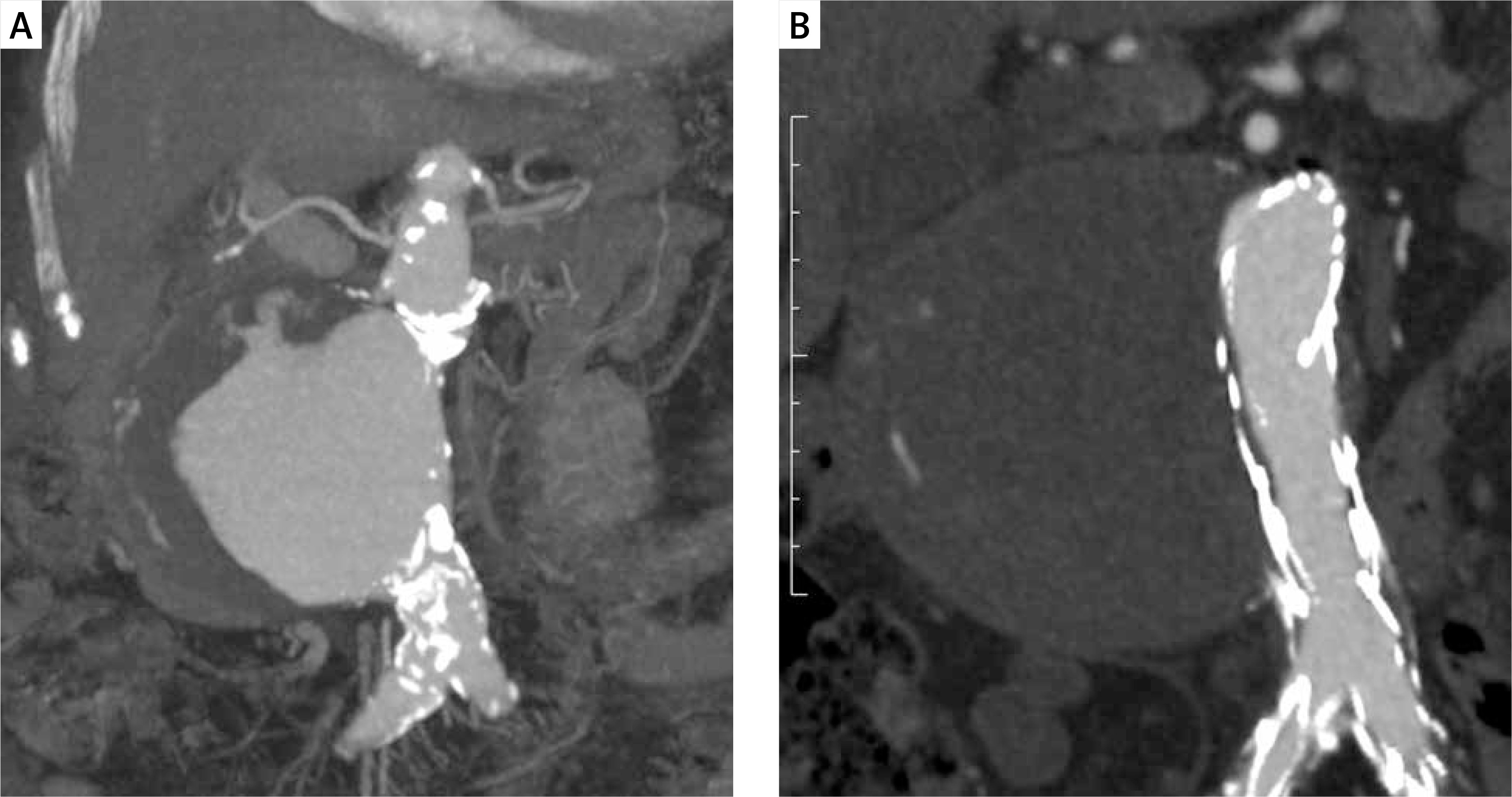
Computed tomography angiography (CTA) revealed the presence of a large saccular aneurysm of the abdominal aorta with a maximal diameter of 111 mm. The neck of the aneurysm was 12 mm long and slightly tapered with a maximal diameter of 20 mm (Figure 1).
Figure 1
Preoperative computed tomography angiography showing a large, saccular abdominal aortic aneurysm (A). Computed tomography angiography performed 10 months after the implantation of the AFX 2 endoprosthesis showing successful exclusion of the aneurysm from the circulation (B)
Echocardiography showed the presence of bicuspid aortic valve and severe aortic stenosis with a mean pressure gradient of 43 mm Hg. There was hypertrophy of cardiac muscle. The ejection fraction of the left ventricle was 55%.
Due to the severe aortic stenosis, the patient was deemed unfit for any aortic intervention. Because of the symptomatic nature of AAA, it was decided to perform a simultaneous BAV and EVAR.
The procedure was performed in a hybrid operating room under general anaesthesia using a fluoroscopic interventional system (Azurion Clarity IQ, Koninklijke Philips N.V., Netherlands). After the patient was anaesthetised an endocavitary electrode was placed through a right jugular vein in the right ventricle. Then, the BAV was performed through a surgically exposed right common femoral artery. The stenotic aortic valve was crossed with a 0.018” guidewire and Vert 5F catheter. The 0.018” guidewire was exchanged for an Amplatz Super Stiff guidewire and passage of a 23 mm balloon through the stenotic valve was attempted. Because it was unsuccessful the stenosis was crossed with an 18 mm balloon and dilated. Despite the pre-dilatation with the 18 mm balloon the passage of the 23 mm balloon was no sooner successful when an 80 cm 9F introducer sheath was used as a support. Using the rapid ventricular pacing of 150/min, 3 sequential successful inflations of the 23 mm balloon at the level of aortic stenosis were performed. After the procedure the patient was stable, with a heart rate of 76/min and blood pressure 100/60 mm Hg.
Then, EVAR with an AFX Endovascular AAA System (Endologix LLC, Irvine, California, USA) was performed. Through the right common femoral artery, a 17 French AFX Introducer was advanced into the abdominal aorta, and a 7 French introducer was inserted percutaneously into the left common femoral artery. An AFX2 bifurcated stent graft of 22 mm diameter and aortic length 100 mm was introduced through the right common femoral artery, and after snaring of the contralateral limb, it was deployed in the abdominal aorta. The orifices of the renal arteries were visualised on the arteriography and a VELA suprarenal endograft of diameter 25 mm and length 95 mm was introduced and deployed. The sealing zones were moulded with a complaint balloon. The completion arteriogram showed very good apposition of the elements of the endograft within the aneurysmal neck without endoleak. The total dose area product and total air kerma were 514.6 Gy cm2 and 1471 mGy, respectively. Both the procedure and the postoperative course were uneventful. After the procedure the patient was in good condition, without clinical symptoms of aortic stenosis. Postoperative echocardiography, which was done 5 days after the procedure, showed markedly decreased pressure gradient at the aortic valve to 38 mm Hg, corresponding to a moderate aortic stenosis. Postoperative course was uneventful, and the patient was discharged home. At 1 year follow-up she was alive, in good general state. On the control abdominal CTA performed 10 months after the procedure the stentgraft was patent with no evidence of endoleaks. The aneurysmal sac was thrombosed with a maximal diameter of 111 mm (Figure 1). Her renal function was stable with a serum creatine of 1.07 mg/dl and eGFR of 51.4 ml/min/1.73 m2. Her exercise tolerance remained improved with a B-type natriuretic peptide concentration of 44.3 pg/ml.
This report presents a case of successful simultaneous management of large, symptomatic abdominal aortic aneurysm, and severe aortic stenosis. The size of the aneurysm, its saccular morphology, and symptomatic presentation undoubtedly signified a high risk of rupture. As well as the aortic aneurysm, the patient also had a severe aortic valve stenosis that markedly increase the risk of non-cardiac intervention.
Although the aneurysmal neck anatomy was suboptimal, in view of high cardiovascular risk, the choice of EVAR for the repair of the AAA in this patient seemed obvious. The 30-day mortality after EVAR is around 1.5% while open surgical repair carries a risk of 30-day mortality of around 4.5% [3]. EVAR is considered an intermediate-risk procedure with a combined 30-day death, myocardial infarction, and stroke risk between 1% and 5%, and open surgical AAA repair is considered a high-risk procedure with a combined 30-day death, myocardial infarction, and stroke risk > 5% [4]. That is why endovascular procedures should be considered for patients with high cardiovascular risk undergoing vascular intervention. In patients with severe symptomatic aortic stenosis in need of time-sensitive non-cardiac surgery, BAV performed beforehand may be the option. In this case, because of the urgent indications for the AAA repair, it was decided to perform simultaneously BAV and EVAR. The rationale behind such approach was as follows. First, the delay between the BAV and EVAR was avoided, and we strongly felt that any delay between BAV and EVAR would expose the patient to a high risk of rupture. Moreover, both procedures should preferably be performed in a hybrid operating room, and they can be performed by the same access site, which lowers the risk of access site complications. Such an approach also decreased the risk associated with anaesthesia because the patients underwent one aesthetic procedure instead of 2. There was good cooperation in the centre between the interventional cardiology and vascular surgery teams, which facilitated such an approach.
Due to a short and slightly irregular aneurysmal neck, the AFX endovascular AAA system was chosen for the aneurysm repair, mainly because of the possibility of precise placement of the graft just below renal arteries and good apposition of the stentgraft in the neck area. Moreover, it is relatively simple to implant and requires only a 7 French access on the contralateral side, which limits the risk of complications. It should be mentioned, however, that due to the 12 mm length of the aneurysmal neck the AFX endovascular AAA system was used outside its instructions for use. Although there are devices registered for a 10 mm long neck, they were not used because they were not immediately available and the centre’s experience with those devices was limited. Despite a suboptimal anatomy, good angiographic and clinical results were observed 10 months after the procedure. The aneurysmal sac was thrombosed, and growth of the aneurysm was stopped, the maximal aneurysm diameter stabilized at 111 mm, which is associated with a favourable long-term outcome [5].
Obviously simultaneous performance of 2 complex endovascular procedures increased exposure of the patient to both ionising radiation and contrast media. However, the radiation dose was reasonably low, and the patient did not present any deterministic effects of radiation, and her kidney function did not deteriorate after the procedure.
It can be concluded that simultaneous balloon aortic valvuloplasty and endovascular abdominal aortic repair is safe in a high-risk patient with a symptomatic abdominal aortic aneurysm.