
 ENGLISH
ENGLISH





INTRODUCTION
Glaucoma alongside cataract are the leading causes of loss of vision worldwide. Out of these two, glaucoma vision loss is irreversible. These age-related diseases tend to coexist, thus creating a need for more complex treatment plans for the patients [1]. In case of cataract – the most common treatment method is phacoemulsification surgery while increased ocular pressure in glaucoma can be treated topically or surgically. Over the last few decades lots of different methods have been developed to manage this problem. The list includes classical trabeculectomy, minimally invasive surgeries and numerous implantable drainage devices such as Ex -PRESS, iStent and PRESERFLO [2]. In this study we focus on comparing the Ex-PRESS shunt implantation with trabeculectomy. Previous studies comparing the results and safety profile of these two procedures have been inconclusive on whether any of these methods is superior [3, 4]. We aimed to focus on patients who were in need of both – cataract and glaucoma surgery. Then we compared the outcomes with the results of anti-glaucoma procedures in pseudophakic eyes. There have already been studies that include the comparison for Ex-PRESS implantation [5-7] and trabeculectomy [8-14], however they focus on these procedures separately. There is also a publication concentrating on comparing trabeculectomy combined with phacoemulsification versus Ex-PRESS implantation with phacoemulsification [15], however it proved to be inconclusive and does not contain comparison with the surgeries on pseudophakic eyes. We wanted to conclude whether or not there are any indications for proceeding with each approach.
Trabeculectomy is a well-established method of glaucoma treatment in use since 1968 that has been developed and perfected by Cairns [16]. Its effects and modifications as well as complications are vastly known [2, 17, 18]. Since the introduction of mitomycin-C (MMC) use in trabeculectomy surgeries the method has gained popularity and is broadly used worldwide. It is stated that MMC reduces the chance of bleb failure and improves the intraocular pressure (IOP) control. The indications and possible complications of using MMC have been previously acknowledged [19-22].
Ex-PRESS a non-valved, stainless steel mini-drainage device used for glaucoma management. It is implanted under the scleral flap and channels aqueous humor from the anterior chamber to the intrascleral space [23, 24]. The shunt is available in different versions with an inner lumen of 50 µm (R-50, P-50) and 200 µm (P-200). Indications for the procedure include uncontrolled IOP and exhaustion of available pharmacological and surgical methods. Its efficacy is comparable with trabeculectomy and both have similar profiles of complications including hypotony, bleb leaks, and choroidal effusion. Additional established risk factors for failure of the Ex-PRESS implantation are non-Caucasian race, previous glaucoma surgeries and diabetes [5, 25].
Based on this study, we would like to present the effects and comparisons of all the methods described above with distinction of the anti-glaucoma surgeries performed on pseudophakic eyes and surgeries combining cataract and glaucoma treatment.
Material and methods
Patient selection
The retrospective study included 105 eyes of 77 patients with open-angle glaucoma who underwent trabeculectomy or EX-PRESS shunt implantation as well as phacoemulsification in SPKSO Ophthalmic University Hospital in Warsaw between October of 2017 and August of 2022. The patients included in the study were either pseudophakic or phakic. All the phakic patients underwent concurrent glaucoma and cataract surgery with intraocular lens implantation. Previous ocular trauma and any surgical procedures to the involved eye, besides phacoemulsification, excluded the eye from the study.
Data
The records of all the patients were retrospectively reviewed. All the included data were gathered from paper documentation provided by the SPKSO (Ophthalmic University Hospital in Warsaw, Poland) archive. Review of the records based on previously selected factors was performed by 2 researchers.
Demographic factors included were sex and age. Open-angle glaucoma was another inclusion criteria, distinguishing primary, secondary, traumatic, pigmentary and exfoliative glaucoma. The patient’s intake of antiglaucoma medication prior to the operation was reviewed and its average value was 3 different medications. Additional criterion was iridotomy preceding surgery.
Complications after cataract surgery were gathered in a group of patients who underwent phacoemulsification prior to glaucoma operation. The study covered a follow-up period of 12 months, within which data concerning BCVA (Snellen chart) and intraocular pressure (IOP, measured using Goldmann applanation tonometry) were collected. All patients were examined on the day preceding the surgery, day 1, day 3, week 2, week 3, month 3, month 6, month 12. Possible complications included in the study and examined during follow-ups were bleeding into the anterior chamber, hypotonia, choroidal detachment, retinal detachment, increase of IOP, filtering bleb leak and uveitis.
Additional medical procedures performed in the postoperative period covered eyeball massage, suturolysis, rinsing the anterior chamber, glucocorticosteroids (GCs) administration, surgical plasty of filtering bleb, laser hyaloidotomy, reoperation, systemic administration of osmotically active drugs, topical administration of drugs lowering IOP and 5-fluorouracil (5FU) Sub-Tenon administration.
The choice of surgical procedure depended on the individual predisposition of each patient. Surgical methods included phacoemulsification with the following Cairns method of trabeculectomy with usage of mitomycin C or Ex-PRESS shunt implantation or concurrent glaucoma and cataract surgery. The version P200 of ExPress shunt was implanted in all cases.
The patients were divided in groups based on the type of procedure they have undergone and then assessed separately. We distinguished 4 groups – trabeculectomy in pseudophakic eyes group (group T), Ex-PRESS in pseudophakic eyes group (E group), phacoEx-PRESS group (PE group) and phacotrabeculectomy group (PT group).
Results
Patient demographics
We analyzed the results of glaucoma operations in 105 eyes of 77 patients diagnosed with primary or secondary open-angle glaucoma. The trabeculectomy group (group T) consisted of 40 eyes, Ex-press group (E group) included 10 eyes, phacotrabeculectomy group (PT group) included 42 eyes and phacoEx-PRESS group (PE group) consisted of 13 eyes. Forty-eight right eyes and fifty-seven left eyes were treated. The average age in group T was 72.12 ±11.27, in group E 70.7 ±11.32, in group PE 68.84 ±13.08 and in group PT 72.69 ±8.32. Patient demographics at baseline and additional data regarding type of glaucoma and number of antiglaucoma medications used prior to surgery are shown in Table I.
Table I
Patient demographic at baseline
Best corrected visus acuity
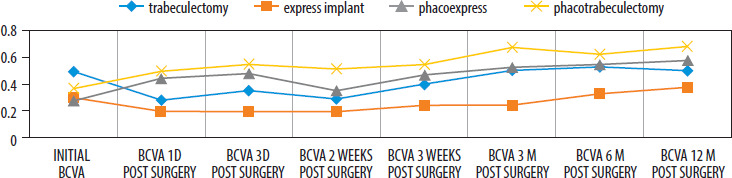
Best corrected visus acuity (BCVA) was measured before treatment, after 1 and 3 days, 2 and 3 weeks, 3, 6 and 12 months. The detailed data are shown in Figure 1. The study came out with a statistically significant difference between the initial and last BCVA (after 12 months) for the group PE and group PT, respectively p = 0.008 and p = 0.00004. BCVA change in the E and T group was not significant (p = 0.222 and p = 0.876). Due to the nature of the procedures, operations performed on pseudophakic eyes (group T and E) and combined glaucoma and cataract procedures (group PE and PT) were compared with each other. No statistically significant differences were observed. The greatest success in improving BCVA over 12 months was observed in the PT group, where 83% of eyes showed improved visual acuity compared to baseline values. In comparison, the improvement in visual acuity in the T, E and PE groups was 43%, 50% and 77%, respectively.
Intraocular pressure control
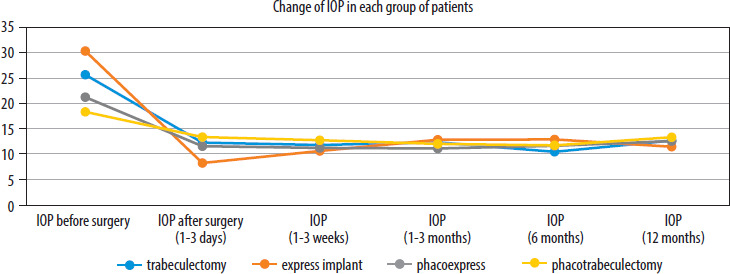
The intraocular pressure control (IOP) control consisted of its cyclic measurements using Goldmann applanation tonometry over a 12-month follow-up. The data from these measurements are shown in Figure 2. The mean intraocular pressure before treatment measured was 25.6 mmHg, 30.1 mmHg, 21.08 mmHg, 18.26 mmHg for the trabeculectomy, Ex-press, phacoEx-Press and phacotrabeculectomy groups, respectively. Based on the result of the t-test, there is a statistically significant improvement in the IOP values received as early as 3 days after the treatment, which is maintained until the end of the scope of this study. For each group the p-value of initial and last measurement was < 0.05 (the p-value was calculated using a t-test giving the following results: pT: p = 0.000000003, pE: p = 0.005598, pPE: p = 0.00209, pPT: p = 0.000003782). The final mean pressures were 12.56 mmHg, 11.4 mmHg, 12.125 mmHg and 13.26 mmHg for the T, E, PE and PT groups, respectively. Comparing the groups with each other, a statistically significant difference was discovered between the results of the group that underwent the Ex-Press implant procedure with the group that underwent trabeculectomy, in favor of the E group (p = 0.034). No differences were observed between the other groups in terms of IOP changes. Comparing the final results of each group with each other, the following results were obtained, 0.38577 for T vs. PE, T vs. PT 0.10371, E vs. PE 0.21796, E vs. PT 0.4035, PE vs. PT 0.45941.
Complications
Complications occurred in all groups. Percentage data on the incidence of individual complications after the procedures are shown in Table II. The lowest percentage was observed in the phacoEx-PRESS group, with 23.1% of patients with any complications, followed by the phacotrabeculectomy group, with 28.6%. The most common complication was an increase in IOP, hypotonia and bleeding into the anterior chamber. No patients with retinal detachment, uveitis or filtration bleb leakage were observed in this study. The group with the highest number of patients with more than one complication was the trabeculectomy group, with 12.8% of patients. When comparing the groups with each other in terms of the overall incidence of postoperative complications, statistically significant differences were observed between the group that underwent trabeculectomy and the group that underwent phacoEx-PRESS (p = 0.0418). Complications included anterior chamber hemorrhage, hypotonia and, to a lesser extent, a postoperative increase of IOP.
Table II
Complications after anti-glaucoma surgeries in each group
Additional medical procedures
The number of patients who required additional medical intervention after the procedure varied between the groups. The detailed data are presented in Table III. 70% of patients in the Ex-PRESS group required no further treatment, which was the best result. Also, there were discrepancies in the number of patients who required two or more additional treatments. This was the case for 46.2% of patients in the T group, 31% in the PT group and 15.4% in the PE group. None of the patients in group E required more than one follow-up procedure. In all groups, the most common additional procedure was eyeball massage. Another common procedure that had to be implemented was suturolysis, with the highest percentage in the trabeculectomy group. The need for the other listed procedures was significantly lower. Topical administration of IOP-lowering drugs was necessary in the PE, PT group and T group. The timing of the inclusion of these drugs varied significantly among all patients, ranging from 2 weeks through 6 months to as much as 12 months after surgery. In these five individual cases, there was a need to implement 3 or even 4 topical IOP-lowering drugs within 12 months after the surgery. Surgical revision of the filtering bleb was performed only in the T group, while reoperation was required by one patient in the PE group and one patient in the PT group. There have been isolated cases of an anterior chamber rinsing, GCs administration and systemic administration of osmotically active drugs. None of the patients included in this study required laser hyaloidotomy. Statistical analysis showed no significant differences in additional medical procedures needed after surgery.
Table III
Percentage of the additional medical procedures performed in each group
Discussion
Among many authors who previously decided to compare either trabeculectomy and Ex-PRESS procedure or performing the surgeries simultaneously rather than separately from phacoemulsification, most found no significant differences, which is coherent with our study. There are some discrepancies between individual researchers, however, in the final conclusions there is no unequivocal argument for any approach. While interpreting the results of these papers, it is important to note that the improval of BCVA in studies that took into consideration procedures combined with phacoemulsification is mostly due to the replacement of the lens rather than the additional effect of anti-glaucoma surgery. Another thing to consider is the existence of previous comorbidities and how that affects the final results of the surgeries. In a study published by Agarwal et al. [22] there was a correlation between present risk factors and the decrease of the surgical success rates. Another notable finding was additive effect of plural comorbidities in one patient on the outcomes.
Authors who focused on comparing trabeculectomy with phacotrabeculectomy have obtained somewhat divergent results. Ahmadzadeh et al. [8] stated that postoperative IOP is comparable and the risk of complications is lower in phacotrabeculectomy, while Takihara et al. [12] observed higher IOP in trabeculectomy in pseudophakic eyes but there were no distinctions in secondary outcomes. Marchini et al. [1] however claimed that it could be beneficial to combine the surgeries when both cataract and glaucoma are advanced enough to be vision impairing. In the study published by Torres-Costa et al. [15] there were no statistically significant differences.
There is less data on Ex-PRESS procedure, yet researchers who studied this surgery opposed to one combined with phacoemulsification gathered similar results. Kanner et al. [7] came to the conclusion that the Ex-PRESS implant is well–tolerated and efficient in each approach. According to Graffi et al. [6] combining the surgeries can lead to excessive anterior chamber inflammation, nevertheless it does not affect the final IOP or the BCVA.
Comparison between trabeculectomy and shunt procedures including Ex-PRESS implant was more frequently included in the papers published in recent years and has mostly consistent results. Wang et al., Gedde et al. and Armura et al. [4, 26, 27] all came to the conclusion that the risk of complications is slightly higher in trabeculectomy groups, especially in the early postoperative phase. The longer was the follow-up, the more similar were the results and long term risks associated with both surgeries. Another coherent point was no overall difference in IOP and BCVA, however it is worth mentioning that the study presented by Arimura et al. [27] mentions higher risk of cataract progression in the trabeculectomy group compared with Ex-PRESS group, which could be indication for either combining trabeculectomy with phacoemulsification or opting for Ex-PRESS procedure in patients with crystalline lens. Nonetheless, Moisseiev et al. [3] points to the high cost of Ex-PRESS implantation as opposed to trabeculectomy, while the presented results do not differ on efficacy and safety profile. All these results are in line with the findings of our study.
The study that focused on inspecting combined approaches was published by Zhang et al. [15] and the main conclusion was that even though there were no statistical differences in the final IOP phacoEx-PRESS may be the preferred and more potent treatment method for patients with coinciding POAG and cataract. This conclusion was made due to the fact that phacoEx-PRESS generated less inflammation and better filtering bleb than phacotrabeculectomy. While current literature points to Ex-PRESS implantation combined with phacoemulsification as a reasonable alternative option to phacotrabeculectomy, the data on the subject is still limited and all indications need to be examined carefully, which was an additional point made by Marchini et al. [1]. Another limitation is the lower availability of this procedure which could potentially lead to progression of the diseases during the elongated waiting time, while there were already well-established methods that are more accessible for patients.
Limitations
This study has several limitations, most important of which is rather vast difference between the number of patients included in compared groups. This is due to relatively narrow indications for performing Ex-PRESS procedure as a first approach and in this study patients with previous anti-glaucoma procedures were excluded. Another is different follow-up time for patients which is a result of hindered access to health care during the COVID-19 pandemic. Lastly, all the records were screened retrospectively which could mean some of the data were incomplete due to lack of prior standardization.
Conclusions
All of the reviewed methods proved to be effective and safe for patients in terms of managing glaucoma.
Performing anti-glaucoma procedures on pseudophakic eyes does not lower the chance of achieving optimal IOP nor does it affect BCVA.
Combining both treatments could be beneficial as there was no significant difference in incidence of complications nor necessary additional medical procedures compared with separate surgeries.
There is still a need for more extensive studies based on a larger group of patients to reach a consensus regarding the safest and most effective approach in treating this frequently co-occurring diseases.