




Introduction
Emergent surgical repair of DeBakey type I and II acute aortic dissection (AAD) aims to prevent potentially lethal complications including stroke, acute aortic regurgitation, aortic rupture into the pericardial space, or myocardial infarction due to dissection of the coronary artery ostia. The increased extent of acute aortic dissection and the consequently a possible preoperative multiple-organ malperfusion can lead to a drastic increase in operative risk. In fact, even with prompt surgical repair, AAD continues to be associated with an in-hospital mortality rate of 20–30% [1–4], and malperfusion of various organ systems can dramatically reduce the chance of a successful outcome [5–9].
Aim
The aim of this study was to evaluate the effect of the extension of aortic dissection according to DeBakey classification, i.e. type I and II, and the relationship with preoperative peripheral and cardiac malperfusion on the early outcome at 60 days after surgical repair in our referred centre for AAD surgery, and at a mid-term follow-up period of 5 years.
Material and methods
Population
A total of 135 patients (mean age: 64.2 ±12.5, range: 24–88, years; males/females: 98/37) who underwent AAD surgery between January 2015 and October 2019 at the referred centre for AAD surgery of the Tor Vergata University Hospital, were analysed. The study was approved by our local Institutional Review Board, which waived the need for patient consent. All patients gave their informed surgical consent. The study was designed to be retrospective.
Diagnosis of preoperative peripheral and myocardial malperfusion was based on clinical symptoms and/or imaging evidence, i.e. absence or reduction of organ perfusion as determined by computed tomography-scan angiography and/or by laboratory enzymes or creatinine serum level, signs of myocardial ischaemia as detected by electrocardiography (ECG), laboratory exams, or by trans-oesophageal echocardiography. Malperfusion was classified as cerebral in the presence of a stroke leading to brain function deterioration; as renal in the presence of an impairment of renal function, i.e. oliguria or anuria requiring continuous veno-venous haemofiltration, or a two-fold increase of creatinine serum level; as visceral if there was evidence of abdominal tension or intestinal dysfunction, increased serum levels of liver and/or pancreatic enzymes; as myocardial or cardiac if creatin kinase MB and troponin I levels were above normal values, i.e. CK-MB/CK-total ratio > 10%, troponin value above 10 ng/ml. In particular, the effect of renal, visceral, and cardiac malperfusion on patient outcome was examined, given their higher incidence at the time of admission at our centre.
Surgical techniques
In the operating room, prior to operative procedures, patients were monitored with Swan-Ganz pulmonary artery catheter, arterial cannulations, i.e. radial and femoral, to ensure continuous arterial blood pressure measurements and corporeal temperature, i.e. rectal, oesophageal, or tympanic measurements during surgery. Additionally, cerebral monitoring was performed with near-infrared spectroscopy (INVOS® System, Somanetics Corp., Troy, MI, USA) and transcranial Doppler measurement of blood flow velocities in the middle and/or anterior cerebral arteries of the Willis circle during the hypothermic circulatory arrest and selective antegrade cerebral perfusion. The heart was accessed through a complete median longitudinal sternotomy. Arterial access for cardiopulmonary bypass was through either the right axillary artery (n = 96) (71%), the femoral artery (n = 32) (24%), or direct aortic cannulation (n = 7) (5%). Aortic repair was performed in conditions of circulatory arrest and moderate hypothermia (24–28°C) in 124 (58%) patients. Cerebral perfusion was given in 104 (77%) cases; of them, 57 (55%) patients received bilateral perfusion according with the Kazui technique [10], and 47 (45%) received unilateral selective antegrade perfusion across the right axillary artery in the right common carotid artery [11]. Three regions of the aorta (ascending, arch, and proximal descending tract) were investigated in each patient to identify sites of intimal tearing; tears were resected whenever possible.
Data collection
In-hospital mortality included both intraoperative and postoperative mortality within 60 days of surgery. Causes of death were described. Clinical follow-up visits were performed every 12 months in our outpatient control unit; computed tomography (CT)-angiography scan and or echocardiographic data were collected. For patients living far from this institution, who could not participate in regular follow-up visits to the department, clinical status was ascertained by personal interviews with the patients and their cardiologists. Causes of death, survival, freedom from cardiac death, freedom from new vascular interventions, i.e. thoracic endovascular aortic rep air (TEVAR), into the distal aorta, and redo operation procedures were recorded.
Statistical analysis
Statistical analysis was performed using Stat View 4.5 programming (SAS Institute Inc., Abacus Concepts, Berkeley, CA, USA). Student’s t-test for continuous variables and χ2 or Fisher’s exact tests for categorical variables were used. To detect independent predictors of 60-day postoperative mortality, logistic regression analysis was performed. Statistical significance by univariate analysis at a p-value < 0.1 was required for entry into the multivariate model. Preoperatively analysed variables included age, gender, arterial hypertension, smoking status, body mass index, body surface area, history of concomitant coronary artery disease, diabetes, chronic kidney disease, previous cardiac surgery, left ventricular dysfunction, extent of the dissection, i.e. type I and II AAD according with DeBakey classification, presence and type of preoperative peripheral and or cardiac malperfusion, cardiac tamponade, and site of entry tear. Intraoperative analysed variables included cannulation site, techniques to obtain brain perfusion, surgical times, whether there was a need for circulatory arrest, and type of operation, i.e. isolated ascending aorta replacement extended to hemiarch only, Bentall procedure, and total arch replacement. Mid-term survival, not including 60-day postoperative mortality, and freedom from late cardiac death were expressed as a mean of the values plus or minus 1 standard deviation. Survival analyses were computed using the Kaplan-Meier method; the Mantel-Cox log-rank test was used to compare survival estimates between subgroups. The Cox regression model was used to evaluate the influence of the analysed variables on time to death and time to requirement of a new treatment for distal aorta. In particular, the extent of dissection, i.e. type I or II AAD, and the presence of preoperative peripheral and cardiac malperfusion on these 2 outcomes in the mid-term follow-up were analysed. Statistical significance by linear Cox analysis at a p-value < 0.1 was required for entry into the Cox regression model. All p-values less than 0.05 were considered statistically significant.
Results
In-hospital results
In total, 103 (76.3%) patients were affected by DeBakey type I AAD, and 32 (23.7%) by type II AAD. Fifty-six (41.5%) patients preoperatively showed peripheral malperfusion, i.e. renal, visceral, neurological, myocardial malperfusion, or both. In the context of peripheral malperfusion, renal, with or without associated visceral, was prevalent (Table I). Cardiac tamponade or pericardial blood effusion was detected by means of computed tomography-scan and/or transoesophageal echocardiography in 71 (52.6%) patients. All preoperative patients’ characteristics are reported in Table I.
Table I
Preoperative characteristics (135 patients)
| Parameter | Value |
|---|---|
| Age [years], mean value ± SD | 64.2 ±12.5 |
| Age > 75 years, n (%) | 33 (24.4) |
| Male/female, n (%) | 98/37 |
| Body surface area [m2], mean value ± SD | 1.94 ±0.23 |
| Body mass index, mean value ± SD | 27.0 ±4.98 |
| Obesity*, n (%) | 35 (25.9) |
| Hypertension, n (%) | 111 (82.2) |
| Smoking habit, n (%) | 32 (23.7) |
| History of cardiovascular disease, n (%) | 16 (11.9) |
| Diabetes, n (%) | 11 (8.14) |
| Previous cardiac surgery, n (%) | 8 (5.93) |
| Cardiac tamponade, pericardial effusion, n (%) | 4 (1.80) |
| DeBakey type I aortic dissection, n (%) | 103 (76.3) |
| DeBakey type II aortic dissection, n (%) | 32 (23.7) |
| Malperfusion (overall), n (%): | 56 (41.5) |
| Cardiac | 11 (8.14) |
| Cerebral | 1 (0.74) |
| Renal ± visceral | 43 (31.9) |
| Limb | 1 (0.74) |
| Port entry of the dissection, n (%): | |
| Aortic root | 14 (10.4) |
| Ascending aorta | 87 (64.4) |
| Arch | 21 (15.5) |
Intimal tearing occurred in the aortic root with coronary ostium/a involvement in 14 (10.4%) patients, in the proximal ascending aorta in 87 (64.4%) patients, in the arch in 21 (15.5%), and in the descending aorta in 5 (3.7%); in 8 (6%) patients no entry tear was found. Sixty-four (47.4%) patients underwent isolated ascending aortic replacement plus or minus hemiarch resection; the aortic root was replaced in 49 (36.3%) patients using the modified button Bentall operation plus or minus hemiarch resection, and 22 (16.3%) patients underwent both total arch and ascending aorta replacement with or without Bentall operation. Mean duration of cardiopulmonary bypass, aortic cross-clamp, and, when performed, circulatory arrest times were 206 ±83, 110 ±47, and 32 ±29 minutes, respectively. Associated coronary artery bypass was required in 12 (8.9%) patients.
Intra-operative mortality was 11% or 15/135 patients; in 9 of them it was due to acute heart failure, and in 6 due to massive bleeding. Postoperative 60-day mortality was 20.9% or 26/124 patients. Causes of death were cardiac in 7 patients, i.e. low output syndrome, n = 6, sudden death, n = 1; postoperative malperfusion syndrome and multi-organ failure in 9 patients; respiratory failure in 6; stroke in 2; and sudden rupture of the aorta in 4, i.e. at the anastomosis site after Bentall operation, n = 1, in aortic arch, n = 1, in descending aorta, n = 2.
DeBakey type AAD; preoperative malperfusion
Preoperative cardiac malperfusion was present in 21.9% or 7/32 patients affected by DeBakey type II AAD and in 16.5% or 17/103 patients affected by DeBakey type I AAD (p = NS). As compared with type I AAD, postoperative peripheral (6.25% vs. 46.5%; p < 0.01) and cardiac (12.5% vs. 28.1%; p = 0.05) malperfusions were significantly lower for type II AAD. There was a significant linear correlation between the preoperative and the postoperative peripheral malperfusion (p = 0.01). As compared with type I AAD, type II AAD patients experienced very significant lower intra- (0% vs. 14.6% or 15/103 patients; p < 0.05) and postoperative (3.1% or 1/32 patients versus 28.4% or 25/88 patients; p < 0.001) mortality rates. Postoperative mortality was higher after total arch and ascending aorta replacement with or without Bentall operation, in comparison with that observed after isolated ascending aortic replacement plus or minus hemiarch resection and Bentall operation plus or minus hemiarch resection (54.5% or 12/22 patients vs. 36.7% or 18/49 patients, vs. 17.2% or 11/64 patients; p = 0.002). Risk factors for mortality identified in univariate analysis are reported in Table II. In the logistic regression analysis a protective factor of intra- and postoperative mortality was type II AAD (RR = 0.03, p = 0.001); independent predictors were hypertension (RR = 7.54; p < 0.01), preoperative cardiac malperfusion (RR = 3.54, p = 0.05), and preoperative renal-visceral malperfusion (RR = 3.94, p = 0.01) (Table II).
Table II
Risk factors and independent predictors of postoperative mortality
Mid-term follow-up results
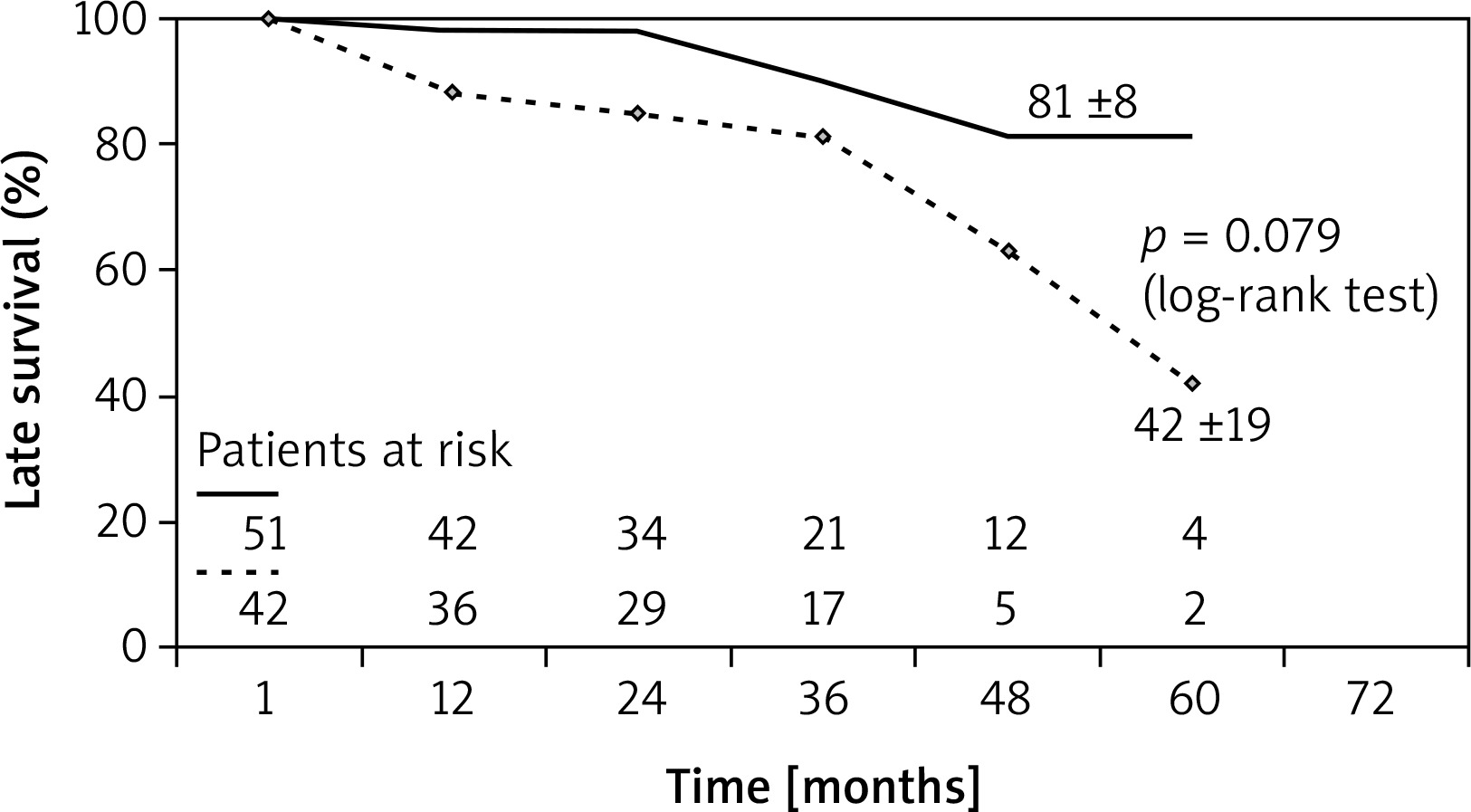
The status of patients was ascertained during a 2-month period (March-April, 2020). Patients were followed for 31.5 ±16 (range: 4–63) months; median 31 months. Four patients were lost to follow-up, and follow-up was 96% complete. At 5 years, overall survival was 74 ±6.9%. The late death rate was 15.6% or 15/94 patients: 9 patients died for non-cardiovascular causes, 3 for cardiovascular causes, i.e. 2 sudden death, 1 rupture of aorta, 1 septic shock, and 2 unknown. Based on the Cox regression analysis, independent predictors of reduced survival were the major extension of type I AAD into the thoracic-abdominal segment of the aorta (RR = 5.37, p < 0.05) and the preoperative cardiac malperfusion (RR = 5.78, p < 0.05) (Table III). At 5 years, freedom from late cardiac death, redo surgical operation, and new vascular procedures, on the thoracic and abdominal aorta, was 92 ±5.7%, 99 ±1.2%, and 81 ±7.2%, respectively. TEVAR procedures were required in 7 (7.4%) patients on the descending thoracic or abdominal segment of the aorta due to the progression of aneurysmal disease in all cases at a mean follow-up of 30 months; 1 patient required redo surgery due to mediastinal infection. Extension of type I AAD to the thoracic-abdominal aorta was also a predictor of the need for new vascular procedures on distal aorta (RR = 1.66, p = 0.05) (Table III). Kaplan-Maier Log-rank tests showed that 5-year survival was 80 ±12% in patients who were 75 years of age or younger at the time of operation, whereas it was 28 ±22% for those who were older than 75 years (p < 0.01) (Figure 1). The survival rate was 81 ±8.0% for patients not affected by DeBakey type I extending to the thoracic-abdominal aorta and 42 ±19% for those who were affected, although this difference did not reach a statistical significance at the log-rank test (Figure 2).
Table III
Independent predictors of late survival and new vascular procedures on thoracic-abdominal aorta†

Discussion
Despite advances in surgical and anaesthetic management of acute aortic dissection, surgical repair of AAD is still performed with high mortality. According to the International Registry of Aortic Dissection (IRAD), the expected mortality for patients undergoing surgery for acute type I or II aortic dissection varies from 20 to 30%. The mortality rate remains high because, as pointed out by Wang et al. [12], the preoperative presentation of patients in recent years has become increasingly serious, with a higher incidence of single- or multi-organ malperfusion. In our centre, the operative mortality, including intraoperative, was 30%. The analysis of our data highlights some aspects that we would like to emphasize. As expected, the extent of acute dissection limited to the first segment of ascending aorta, type II according to DeBakey classification, was associated with much better immediate postoperative results compared to type I, both in terms of intraoperative and 60-day postoperative mortality. The mortality rate of 3.1% in this group of patients appears to be superimposable to that expected in the operations of ascending aorta repair, both isolated and with Bentall operation, performed in the elective regime, ranging from 2.2% to 4% [13, 14]. In addition, type II AAD was significantly associated with a lower incidence of any postoperative malperfusion, both myocardial and peripheral, thus resulting in a much lower operative mortality. Preoperative malperfusion syndrome increases dramatically in-hospital mortality, up to 80% [5–9, 15, 16]. We performed a retrospective analysis of a single centre with adequate experience in the treatment of acute aortic dissection, paying particular attention to preoperative malperfusion involving specific organs, renal and visceral, and the influence of this complication on the outcome in the short and medium term. In our experience, peripheral preoperative malperfusion of all types, i.e. renal, visceral, others, and cardiac malperfusion, whether associated or not, occurred in 56 patients or in more than 40% of cases, and correlated significantly with the presentation of postoperative malperfusive syndrome. The incidence of postoperative malperfusion was 25/120 patients or 20%, and it was the main cause of death after surgery. Therefore, the surgery allowed the resolution of the malperfusion in about half of the cases, but in the other half, proximal aortic replacement surgery did not provide a prognostic benefit in such patients.
In fact, as on the one hand the minor extension of the dissection of type II at the logistic regression analysis was identified as an independent protective factor of operative mortality (RR = 0.03); on the other hand, preoperative renal-visceral and cardiac malperfusions were detected as very important independent predictors of death, with RR values of 3.94 and 3.54, respectively.
In our study, we detected arterial hypertension as another very important risk factor of operative mortality, with a RR value of 7.54. This finding could be related to the fact that in patients who usually have higher arterial tension values, the presence of systemic hypotension, typical manifestation of type A acute dissection affecting the proximal segment of the aorta, can more easily favour the preoperative onset of malperfusive syndrome in comparison with normotensive patients.
Given the high incidence of preoperative onset of malperfusive syndromes and the high mortality they entail, there is an open debate on the choice of therapeutic strategy to be adopted in these cases [17–22]. That is, if aortic surgical repair is always, in any case, indicated immediately, or if it may be more appropriate to carry out interventional procedures on the false lumen of the aorta to improve the organ’s perfusion before surgery [23–28].
In the discussion on the contemporary treatment of acute aortic dissection, the authors Chen et al. [29] emphasize that the primary purpose of the treatment of AAD is to save the patient, with an intervention on the proximal aorta that should be as short as possible. Moreover, it should be considered that the severity of preoperative malperfusion is not always well known, and that any delay in evaluation may increase the risk of death. However, when dissection affects the left main stem or the right coronary ostium, the authors recommend bypassing the left anterior descending and/or right coronary artery as protection for myocardium. In the presence of a dissected superior mesenteric artery, with a dynamic or static malperfusion detected by the CT-scan, the authors suggest endovascular aortic fenestration/stenting before to open aortic surgical repair. If after mesenteric arterial reperfusion patients develop ARDS, sepsis, or multi-organ failure, in such cases the authors suggest waiting even 2–4 weeks; while, if isolated renal malperfusion is present, the authors suggest immediate surgery [29].
The presence of malperfusion syndrome is associated with the highest operative mortality. Several authors have highlighted q 4- or even 4-fold rise of mortality in the presence of intestinal ischaemia and high lactic acid levels.
Lawton et al. [30], Narayan et al. [31], Feier et al. [32], and Yang et al. [25], in AAD patient populations of 282, 205, 153, of 602 cases, underline that in patients with preoperative lactic acidosis and mesenteric ischaemia, surgical treatment can lead to unacceptable mortality, with a 10-fold rise in mortality-RR values. Therefore, the authors suggest the absolute necessity of a 2-stage treatment to restore in first-stage intestinal adequate perfusion and, subsequently, after improvement of the patient’s general condition, surgical repair of the dissected aorta.
In our study, cardiac malperfusion was responsible of 9 out of 15 intraoperative deaths: it was likely due to the irreversible myocardial injury and the inability to wean off from cardiopulmonary bypass; moreover, cardiac malperfusion has negatively affected also the late survival. Cardiac malperfusion development in the postoperative period had had a strict relation with the DeBakey type I AAD. Our data highlight the importance of a correct diagnosis upon initial presentation. In fact, at admission, the coexisting coronary acute syndrome may be overlooked or misdiagnosed. Such a mistake can lead, after 60 minutes, to the development of serious ischaemic damage to the sub-endocardial myocardium, and after 3 hours to transmural necrosis, inducing both irreversible heart failure and chronic left ventricular dysfunction with a consequent negative impact on mid-term survival, as observed in our study.
Nishigawa et al. [33], comparing early and late outcomes between AAD patients who had preoperatively renal malperfusion (n = 64) and those who did not have this complication (n = 470), found that renal malperfusion was an independent predictor of operative death (OR = 3.08), but it was not associated with higher late mortality. Also in our series, preoperative renal malperfusion was not identified as predictor of late mortality. In the same way, Qian et al. [34], in a population of 208 patients undergoing AAD repair, showed that preoperative kidney malperfusion was an important risk factor for early outcomes, addressing 20.8% incidence of postoperative kidney injury and 22.9% of in-hospital mortality, but not for late death.
IRAD reports have clearly shown the impact of patients’ age at operation on early and late outcomes. Of 2952 patients, mean age 62 ±14 years, affected by type A AAD, 936 were surgically treated, and about one-third of them had age greater than 70 years. In those aged over 70 years, operative mortality was significantly higher, i.e. 38.6% versus 26% in younger patients (p < 0.0001) [35, 36]. Caus et al. [37] showed the negative impact of 70 years of age on the mid-term outcome, especially if, beyond the advanced age, the presence of another risk factor was associated, such as any type of preoperative malperfusion. This finding did not differ from that observed in our study, in which patients aged 75 years had had a significantly lower survival at 5 years in comparison with younger patients, i.e. 28 ±22% vs. 80 ±12%, respectively (Figure 1), and from that analysed in another, previously published series [38].
As well as for the operative results, even for those during the follow-up, the greater extension of DeBakey type I aortic dissection into the thoracic-abdominal segment was associated with a worse prognosis, as demonstrated by significantly lower survival and greater need for vascular procedures on the thoracic and abdominal aorta segments (Tables II, III, Figure 2).
The present study has several limitations. It is retrospective and observational; the analysis of data was focused on examining the impact of the extension of the aortic dissection and, consequently, of the preoperative malperfusion presentation on the early and on the late outcomes, but it was not designed to investigate the therapeutic options for the treatment of the malperfusion. Moreover, in this study we did not carry out propensity-score matching for the adjustment of the patients’ baseline characteristics, in order to evaluate the different preoperative clinical presentation of DeBakey’s type I and II aortic dissection.
Conclusions
As expected, a more favourable anatomy of the type II AAD is associated with a better early and late outcome after aortic repair. This is due to a lower incidence of peripheral and cardiac malperfusion. The latter being the most relevant risk factors for early and late mortality. Type II AAD shows an operative mortality rate comparable to that observed in elective aortic surgery.