




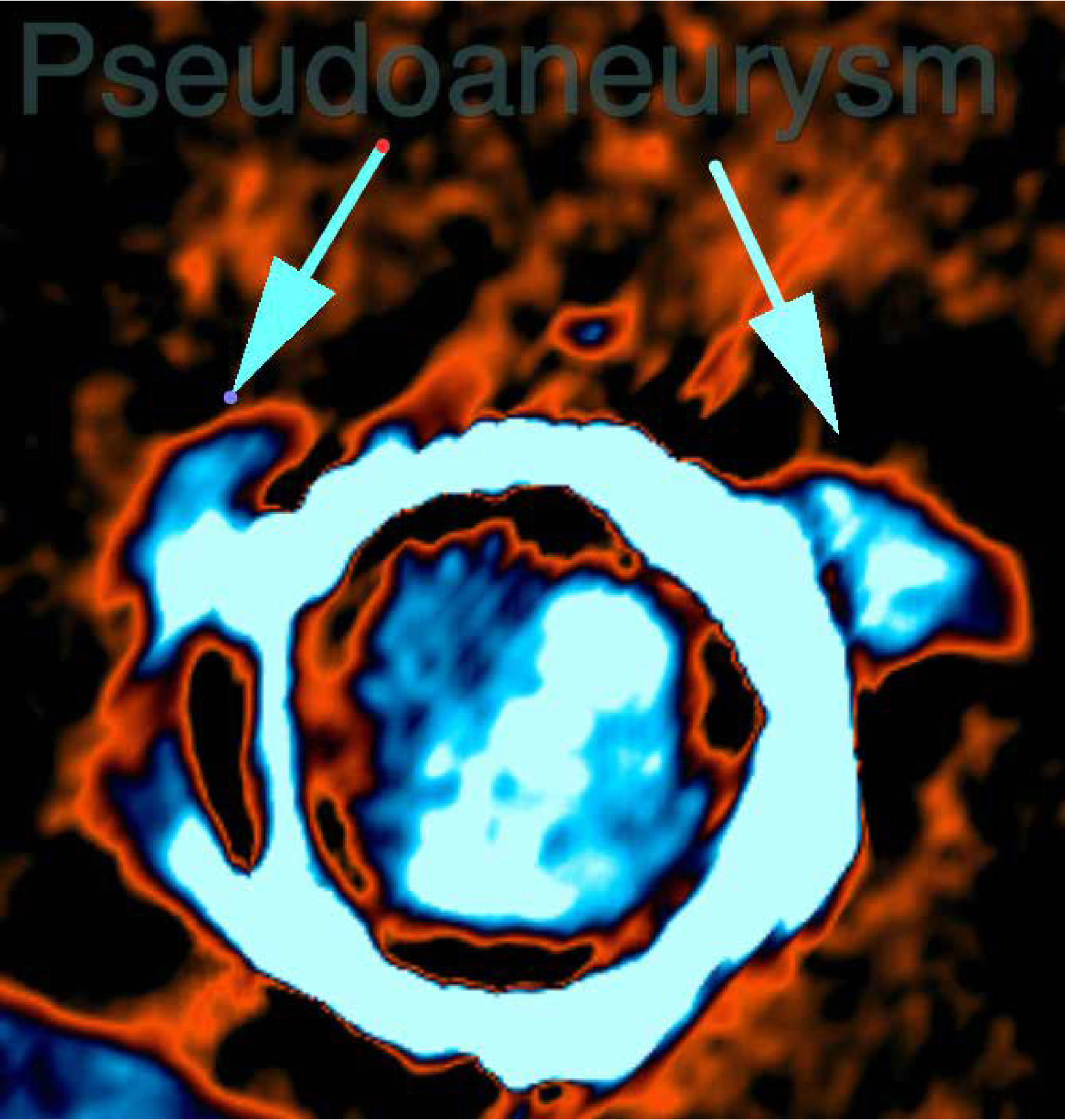
Recently, concerns have been raised about the durability of Mitroflow pericardial bovine cardiac prostheses, particularly with regard to the occurrence of structural valve degeneration (SVD) [1] and a recently published Danish registry reported an increased reoperation rate for the 19 mm and 21 mm sizes [2]. Implantation of a new prosthesis into a small and damaged annulus can be technically challenging and is likely to be associated with high mortality. We reported our experience with implantation of a sutureless Perceval Plus size S aortic valve for structural deterioration of Mitroflow valve with pseudoaneurysms, avoiding debridement of the aortic annulus (Figure 1).
A 72-year-old man underwent aortic valve replacement surgery for failure of the small Mitroflow prosthesis (21 mm). Macroscopic and microscopic examinations of the degenerated prostheses revealed no evidence of endocarditis. The Euroscore II was 9.09% and the STS score was 4.8%. Informed consent was obtained.
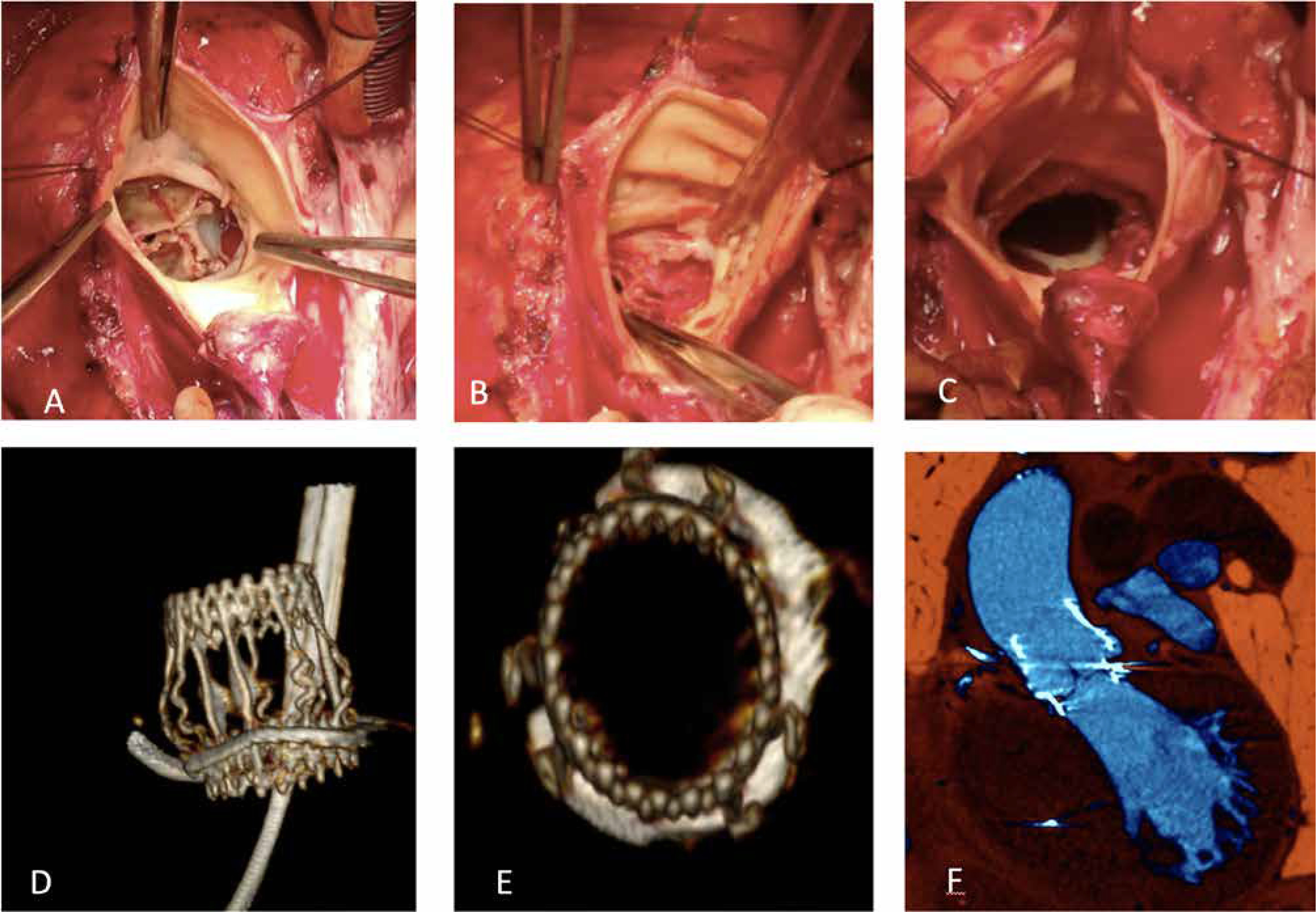
A full median sternotomy was performed. Cardiopulmonary bypass was performed by central cannulation of the ascending aorta and right atrium and the left ventricle was vented through the right superior pulmonary vein. Antegrade crystalloid cardioplegia was administered through the coronary ostia. A transverse aortotomy at least 3.5 cm distal to the aortic annulus was performed and the degenerated prosthesis was completely explanted (Figure 2 A). Pseudoaneurysm repair was performed with a 4/0 prolene running suture (Figure 2 B). To avoid weakening of the annulus, we did not debride the aortic annulus and left the prosthetic ring in place (Figure 2 C). Three 4/0 polypropylene sutures, each 120° apart, were placed in the remaining circular annulus. A sutureless Perceval Plus size S prosthesis was released. The aorta was closed with a 4/0 prolene running suture. Skin-to-skin operation time was 360 minutes, cardiopulmonary bypass lasted 105 minutes and aortic cross-clamping time was 75 minutes. The postoperative course was uneventful. At discharge, postoperative echocardiograms showed good functionality of the Perceval Plus size S prostheses (peak gradient 22 mm Hg, mean gradient 10 mm Hg). A CT scan was performed which showed the good results of Perceval implantation and the absence of any residual pseudoaneurysm (Figures 2 D–F).
Figure 2
Intra-operative images: structural Mitroflow prostheses degeneration (A); pseudoaneurysm (B); aortic annulus (C). Computed tomography scan post-operative images: perceval prostheses implanted inside the outermost part of the Mitroflow prosthetic ring (D–F)
Operative mortality in elective reinterventions of the aortic valve ranges from 2–7 up to 30%. Patients requiring redo valvular surgery are often older and at higher operative risk of adverse events related to concomitant diseases. In addition, repeat surgery is associated with longer cross-clamp and cardio-pulmonary bypass times. On the other hand, implantation of a new prosthesis into a small and destroyed annulus could be technically challenging and is likely to be associated with high residual pressure gradients. Two alternative solutions have been proposed for the treatment of a patient with a failed aortic bioprosthetic valve: transcatheter aortic valve replacement [3] or redo aortic valve replacement [4]. The TAVI valve-in-valve technique has been proposed as a less invasive alternative to open-heart surgery. Nevertheless, transcatheter valve-in-valve implantation in a small degenerated aortic bioprosthesis may be associated with a high residual transvalvular pressure gradient due to the possible underexpansion of the new prosthesis in a small calcified prosthesis and the risk of occlusion of the coronary ostia [5] by the dislodged leaflet of the bioprosthesis.
The sutureless valve in repeat aortic valve replacement appears to be a safe and effective approach that is not associated with high postoperative pressure gradients [6, 7]. Implantation of the Perceval Plus prosthesis in repeat aortic valve replacement has been described associated to aortic annulus debridement. We reported a particular case of Perceval implantation in which debridement of the aortic annulus was avoided and the prosthetic ring was left in place. Before surgery, we performed an experiment with porcine hearts in the laboratory of the University of Tor Vergata in which we implanted a Perceval Plus size S valve into a Mitroflow-21 prosthesis after removing the prosthetic leaflets. We achieved complete expansion of the prosthesis without structural changes. Perceval implantation consolidates the annulus, even if it is fragile and destroyed. This could be an alternative to transcatheter valve-in-vale implantation in complex cases associated with pseudoaneurysm or high risk of coronary artery ostia obstruction.