
 ENGLISH
ENGLISH





In 2016, a 72-year-old man with lesions in the central retina of the left eye presented for an ophthalmic consultation. The patient was in good general condition and was receiving treatment for hypertension, which was well controlled with oral antihypertensive medications.
Approximately 6 months prior, the man had consulted his ophthalmologist because of deterioration of vision in his left eye. At that time, the patient was diagnosed with wet age-related macular degeneration (AMD) in the left eye and was prescribed anti-VEGF therapy. Treatment with aflibercept, administered at the recommended 4-week intervals, was initiated.
Following the second aflibercept injection, there was an unexpected and significant further decline in visual acuity. A subsequent optical coherence tomography (OCT) examination revealed a full-thickness macular hole in the patient’s left eye. It was decided to refer the patient to a specialist vitreoretinal surgeon for a consultation to determine eligibility for surgery.
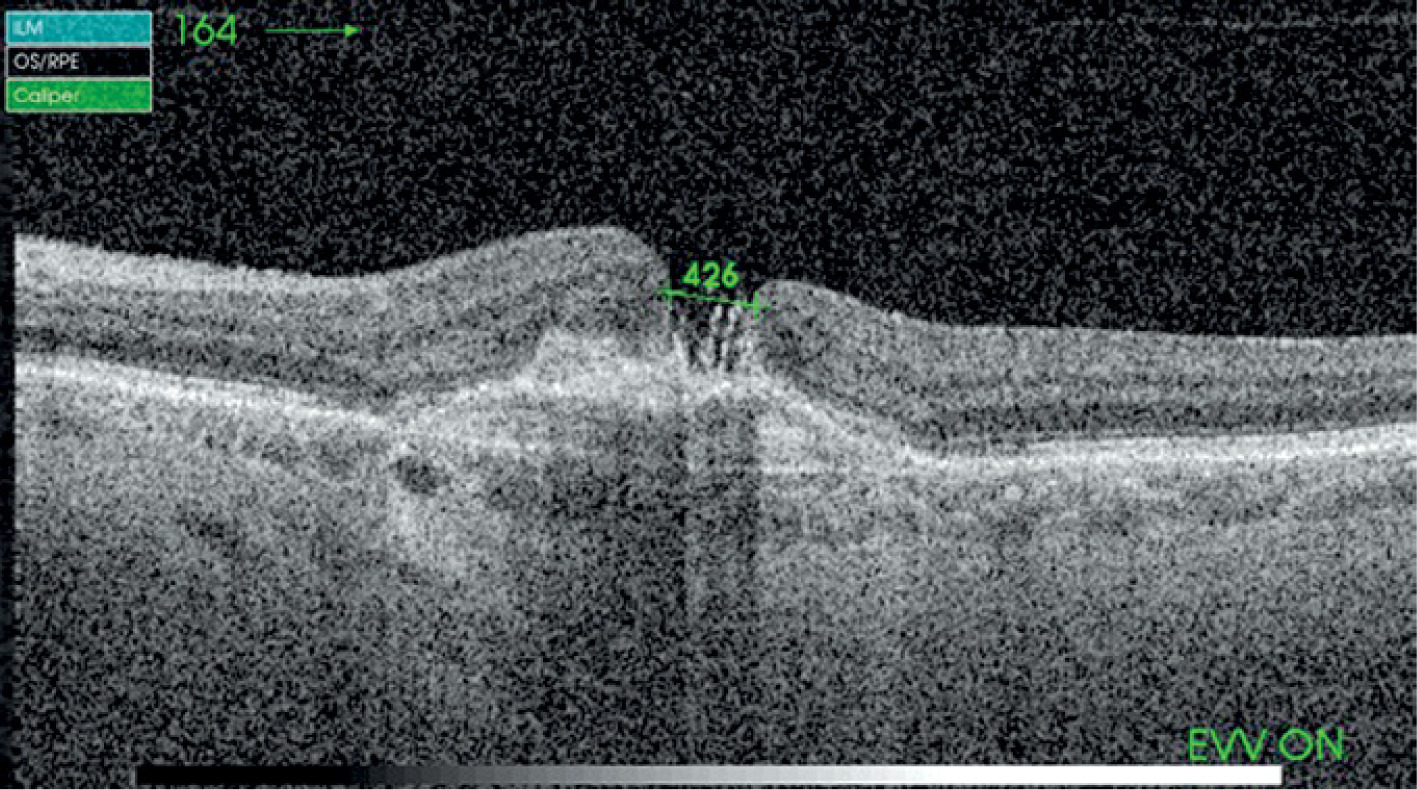
During the surgical consultation, the patient’s visual acuity in the right eye was found to be normal (Vod = 1.0 sc). No abnormalities were observed in the eye fundus either. Furthermore, the examination showed no evidence of active age-related macular degeneration. In the left eye, visual acuity declined to 0.05, and a full-thickness macular hole along with AMD-associated subretinal proliferation were noted. On OCT, the macular hole measured 426 µm in transverse dimension (Figure 1).
Figure 1
OCT examination of the left eye. Full-thickness macular hole and subretinal membrane visible
The patient was provided with information about his ophthalmic condition and the surgical options available for treatment. Alternative therapeutic modalities were also discussed, and it was explained that having two conditions in one eye diminished the likelihood of preserving vision in that eye. The patient was also made aware that even with successful surgery to close the macular hole, the subretinal neovascular membrane associated with AMD would persist in his left eye, necessitating ongoing anti-VEGF treatment.
In the first stage, the cataract was removed. The procedure was performed in a routine manner, without any complications. In the subsequent stage, a 23-gauge vitrectomy was performed. During the procedure, a pre-existing posterior vitreous detachment was found. The internal limiting membrane (ILM) was removed extensively, reaching up to the temporal arcades. Tamponade using 20% SF6 gas was administered. Postoperatively, the patient was instructed to avoid tilting his head upwards for the initial four days.
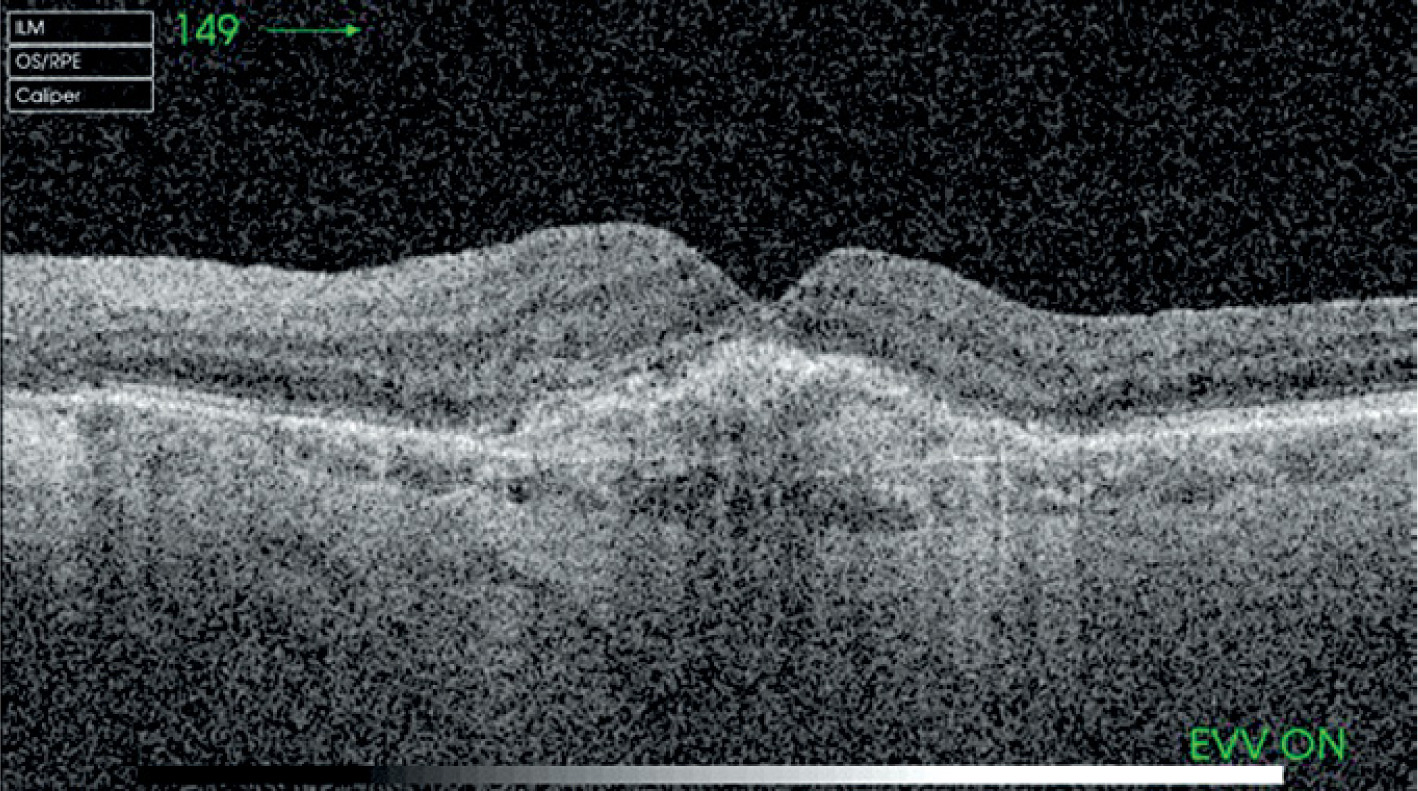
The surgery resulted in successful closure of the macular hole. The retina in this area was altered, with disruption of its normal layered architecture (Figure 2). One month after the surgery, the visual acuity in the left eye was 0.2.
Figure 2
OCT examination of the left eye after surgery. Subretinal neovascular membrane and restored foveal contour visibler
The patient resumed care with the referring physician. Because of persistent wet AMD in his left eye, he was prescribed anti-VEGF treatment again. Following the surgical procedure, from January 2017 to March 2020, a total of 17 aflibercept injections were administered into the left eye. The patient’s visual acuity in the operated eye remains stable at 0.2.
DISCUSSION
Idiopathic full-thickness macular hole is a relatively common condition in ophthalmology. It is more commonly seen in postmenopausal women, likely due to changes in their hormonal balance. A hole in the macula is usually an isolated condition and rarely coexists with other pathologies in the central retina.
Standard treatment involves vitrectomy with removal of the internal limiting membrane and gas tamponade. The specific operative techniques recommended by various experts might vary slightly. There is ongoing debate regarding the optimal extent of ILM peeling and the appropriate type of gas to be used for tamponade. Furthermore, there are differing opinions on whether or not face-down positioning is necessary after the procedure. Also, the inverted ILM flap technique pioneered by Prof. Michalewska and Prof. Nawrocki is increasingly being adopted [1].
In the case discussed here, a macular hole developed during the treatment of wet AMD in an eye with pre-existing subretinal membrane.
Such cases are quite uncommon, and they are not recognized as typical complications of wet AMD [2].
Clinical observations show that not every anti-VEGF injection stimulates a macular hole. Also, idiopathic macular holes rarely occur in coexistence with other pathologies [3]. Central retinal holes may coexist with dry AMD, but in such cases they are typically atrophic and exhibit a different macular hole morphology.
In cases where both a macular hole and wet AMD are present in the same eye, wet AMD typically develops years after performing vitrectomy to treat wet AMD.
In 2004, Tabanadeh et al. published a retrospective study examining the characteristics of subretinal neovascular membranes developing after vitrectomy surgery for macular hole. The study is among the most comprehensive reports on the subject. However, it addresses the development of both conditions in the same eye at separate times, unlike the case presented here, where they occurred concurrently. The authors highlighted the poor visual prognosis in these cases; however, it is important to note that this was before anti-VEGF medications for treating wet AMD were available [3].
The OCT findings in the reported case revealed the typical appearance of the macular hole, with raised and everted edges, accompanied by mild swelling. The morphological features of the hole were consistent with an idiopathic hole rather than an atrophic one, a type more frequently linked to dry AMD. The hole was located entirely on the subretinal neovascular membrane. The direct communication between the neovascular membrane and the vitreous chamber made it difficult to determine whether subretinal fluid had accumulated. The activity of the neovascular membrane prior to surgery was assessed by OCT imaging and clinical examination of the retina. Due to the absence of petechiae or swelling, the subretinal membrane was deemed inactive, and surgery proceeded. The absence of subretinal fluid was considered a positive factor increasing the chances for successful closure of the macular hole.
Vitrectomy was conducted using the standard procedure for an idiopathic macular hole. The preferred surgical method involved removing the ILM as extensively as possible, as close to the vascular arcades as feasible. During the vitrectomy, a substantial portion of the vitreous humor was removed to make room for a large volume of gas. If the eye is filled with approximately 80–90% of gas, face-down positioning is not required for the initial two to three days post-surgery, as merely avoiding tilting the head upwards is sufficient to keep the gas bubble in contact with the macular hole.
The surgery resulted in successful hole closure. The OCT examination showed that the macular structures had been anatomically reconstructed, but the subretinal membrane remained visible due to wet AMD.
The available literature on vitrectomy performed in eyes with coexisting neovascular membranes is rather limited. In 2001, Elsing et al. reported on a vitrectomy procedure designed to close the macular hole and mechanically remove the neovascular membrane [4]. However, other reports and observations show that removing proliferative membranes from beneath the retina does not yield favorable results in terms of preserving visual acuity. This approach was discontinued once anti-VEGF therapy became available.
In the reported case, the surgery successfully resolved the condition. Wet AMD was subsequently managed according to standard treatment protocols. The patient was administered aflibercept every 2 months. No complications or unusual symptoms associated with anti-VEGF treatment were noted. The patient’s visual acuity remains stable at 0.2. The macular hole did not reopen throughout the two-year follow-up period.