
 ENGLISH
ENGLISH




INTRODUCTION
Intraocular infection can be exogenous, occurring after ocular injuries or surgical procedures, or less commonly, endogenous, resulting from blood-borne spread of infection from systemic foci [1-3]. Endogenous causes encompass conditions such as endocarditis, pyelonephritis, pneumonia, arthritis, osteomyelitis, infections of the gastrointestinal and biliary tracts, abscesses in the liver, kidneys, and lungs, and skin infections [1, 2, 4]. Endogenous infections also include those spreading from the immediate vicinity of the eye: the meninges and nasal sinuses.
In cases of endogenous intraocular infection, the most commonly identified pathogens are Gram-positive bacteria (Streptococcus spp., Staphylococcus spp., Meningococcus, Enterococcus spp., Bacillus) and Gram-negative bacteria (Klebsiella pneumoniae, Escherichia coli, Salmonella, Haemophilus influenzae, Neisseria meningitidis) [1-5]. Intraocular fungal infections, typically caused by Candida albicans, occur less frequently and are often complications arising from inserted catheters, cannulas, or prolonged intravenous infusions [1–3]. Unlike bacterial infections, they typically follow a subacute course [1, 2].
Endogenous intraocular infections are associated with sepsis and overall poor health in patients. These factors frequently cause delays in ophthalmological diagnosis, which can lead to a poor visual outcome [1, 4]. In many cases, however, infection arises from asymptomatic or mildly symptomatic bacteremia or fungemia (such as fever or flu-like symptoms), and the primary infection site cannot be retrospectively determined [1, 2, 4, 5].
This report aims to present a case of endogenous endophthalmitis with a very rare etiology, caused by Listeria monocytogenes. It is a Gram-positive, rod-shaped bacterium commonly transmitted through contaminated food, which poses the greatest risk of infection to individuals with impaired immunity. It can be asymptomatic, with estimates suggesting that approximately 10% of the population harbors this pathogen in their digestive system [6]. The gastrointestinal tract is a major natural reservoir for microorganisms which, given favorable conditions, can enter the bloodstream [2]. Listeria monocytogenes also has the capability to spread from the gastrointestinal tract into the bloodstream. Besides endophthalmitis, it can also lead to corneal abscess and encephalitis. Systemic infection carries a high mortality rate of up to 30%. However, when the central nervous system is involved, the mortality rate can increase to as much as 70%. While listeriosis is considered a zoonotic disease, the bacteria responsible for it can also be found in soil and water. The first documented case of L. monocytogenes endophthalmitis was reported in 1967, involving a retired plumber who kept goats and consumed unboiled goat milk [1].
CASE REPORT
A 67-year-old woman, who had been undergoing treatment for IgG κ multiple myeloma for 13 years, including two autologous bone marrow transplants and 5 cycles of intravenous chemotherapy (the most recent cycle completed approximately 1.5 months before the onset of ophthalmic symptoms), was referred to the Department of Ophthalmology at Prof. W. Orłowski Independent Public Clinical Hospital of the Centre of Postgraduate Medical Education (CMKP) in Warsaw on an emergency basis with symptoms of left endophthalmitis. Initially, the patient reported to her local ophthalmology center, complaining of pain, irritation, and reduced visual acuity in her left eye. At that time, anterior uveitis was diagnosed, and local treatment (dexamethasone and tropicamide drops) was prescribed. A follow-up examination 4 days later showed a marked worsening of the local condition in the left eye. Consequently, the patient was referred for further diagnostic evaluation and treatment, with suspected intraocular dissemination of myeloma, to the CMKP Department of Ophthalmology. There, based on the clinical findings, a preliminary diagnosis of infectious endophthalmitis in the left eye, likely of endogenous origin, was made.
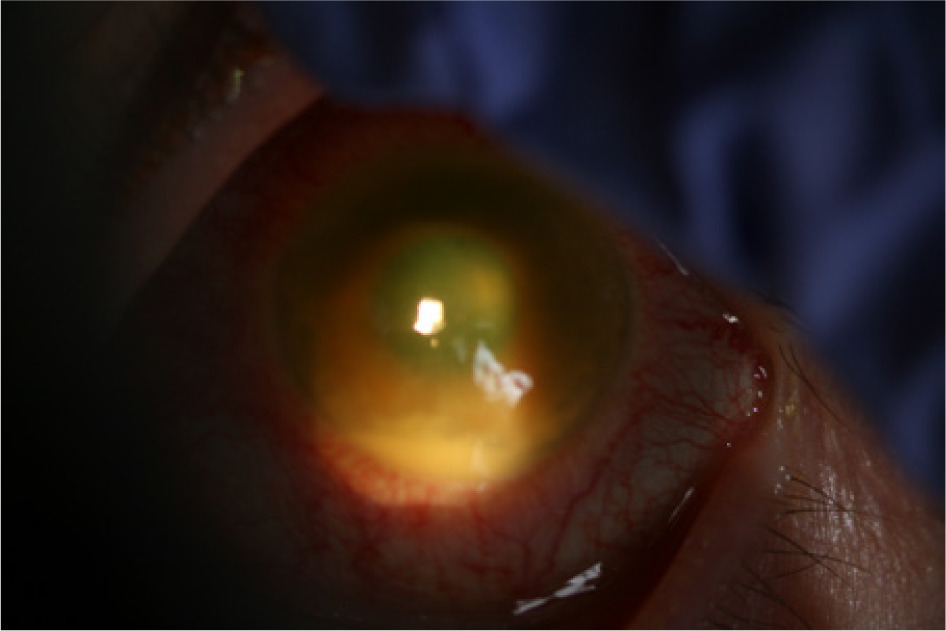
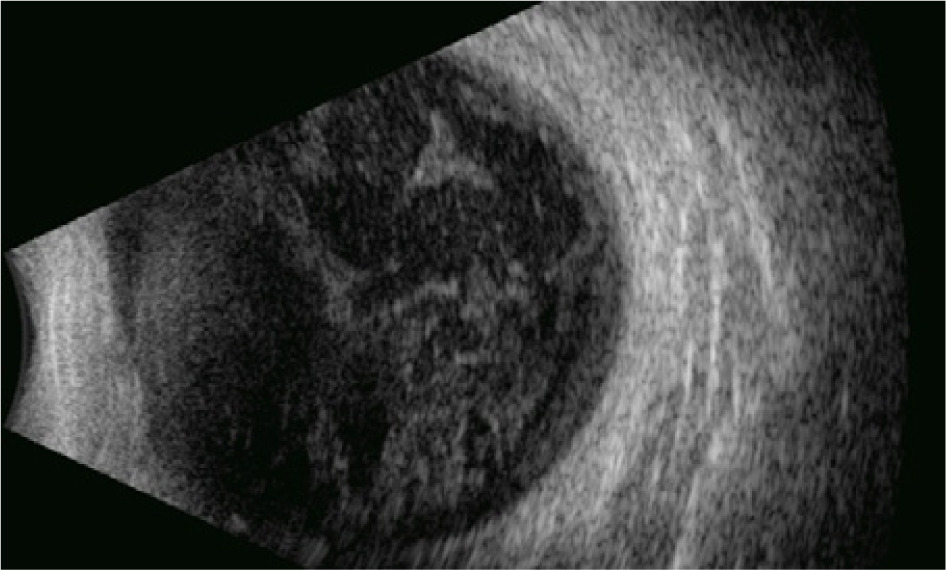
Upon admission, physical examination of the left eye revealed the following: visual acuity was hand motion (HM) with normal light projection, intraocular pressure was normal, the corneal epithelium was swollen with pinpoint erosions and folds in Descemet’s membrane, the anterior chamber was preserved with a 1.5 mm hypopyon, the pupil was non-reactive and exhibited near-complete circular synechiae (Figure 1), and there was inflammatory exudate in the vitreous chamber, obstructing the view of the fundus. Ultrasound imaging showed exudate in the vitreous body and retrohyaloid space, along with retinal adherence (Figure 2). There were no pathological changes in the right eye.
Figure 1
Anterior segment of the patient’s left eye on the day of admission to the Department of Ophthalmology of the CMKP
Blood laboratory tests revealed several abnormalities: elevated ESR of up to 64 mm/h (with only a slight increase in C-reactive protein), leukopenia ranging from 2.67 × 109 to 3.96 × 109 L (which increased during hospitalization; normal range: 4−10 × 109 L), and mild monocytosis of 11.8% (normal range: up to 11%), which further increased to 18.1% during the patient’s hospital stay.
Upon admission, samples of anterior chamber fluid, vitreous fluid, and blood were obtained for bacterial and fungal cultures. An intravitreal injection of vancomycin (1 mg/0.1 ml) and ceftazidime (2.25 mg/0.1 ml) was administered, and empirical intravenous antibiotic therapy with ciprofloxacin (400 mg twice/day) and metronidazole (500 mg 3 times/day) was initiated. Additionally, local medications were prescribed for the left eye: moxifloxacin drops 5 times daily, atropine 3 times daily, and dexpanthenol gel 5 times daily. On the second day of hospitalization, due to elevated intraocular pressure, antiglaucoma medications were introduced, including brimonidine (twice daily) and timolol 0.5% (twice daily). Intravitreal injections of vancomycin and ceftazidime were administered every 2 days (totaling 7 injections during the patient’s hospital stay).
The blood cultures for aerobic bacteria, anaerobic bacteria, and fungi were all negative. The radiological findings of the chest were normal. Abdominal ultrasound examination revealed mild dilatation of the pelvicalyceal system and slit-like calyces. Otherwise, no pathologies were noted. The computed tomography scan of the nasal sinuses and orbits showed minor thickening with subtle soft tissue enhancement near the lateral wall of the left eye after contrast administration.
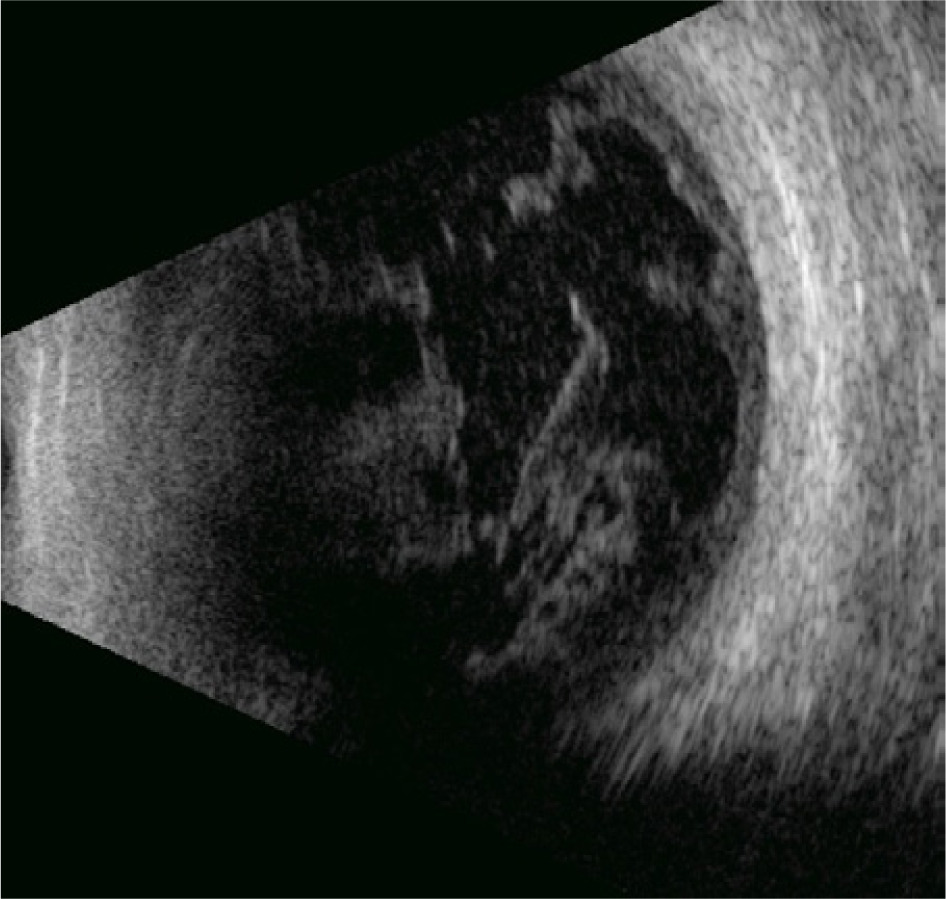
Despite the administered treatment, as described above, there was no clinical improvement. On day 5 of hospitalization, dense fibrin was identified in the anterior chamber of the left eye. Additionally, an ultrasound examination revealed an organized exudate in the vitreous body, which was strongly adherent to the retina. Consequently, the scheduled vitrectomy was cancelled, and instead, the patient underwent anterior chamber flushing followed by intravitreal administration of vancomycin and ceftazidime. On the same day as the procedure, the culture results from the fluid collected from the anterior chamber upon admission were obtained, identifying Listeria monocytogenes. Antibiogram showed susceptibility of the microorganism to penicillin, ampicillin, erythromycin, and trimethoprim/sulfamethoxazole. The systemic treatment was adjusted to incorporate intravenous ampicillin at a dose of 2 g every 4 hours, which is standard for managing central nervous system infections. From day 3 onwards, following the initiation of targeted treatment, clinical examination and ultrasound (Figure 3) showed clear improvement in the patient’s local condition. After 12 days of targeted antibiotic therapy, the patient was discharged from the CMKP Department of Ophthalmology with a distance visual acuity of 0.1 on Snellen charts. Systemic antibiotic treatment with oral ampicillin at a dose of 2 g 6 times daily was continued for additional 2 days. Subsequently, the patient was followed up at the ophthalmology outpatient clinic at her residence. Further improvement in the local condition of the left eye was observed. Five weeks after completing a 2-week course of targeted systemic antibiotic therapy, the patient’s best corrected visual acuity for distance on the Snellen charts was 1.0. By 8 weeks, the anterior segment and fundus appeared normal, with no inflammatory exudate in the vitreous chamber.
DISCUSSION
Endogenous endophthalmitis with a Gram-positive L. monocytogenes etiology is a very rare disease. In a 2014 analysis of 342 cases of endogenous endophthalmitis, only 3% were attributed to L. monocytogenes [7]. In a 2018 review of 43 cases of endophthalmitis with L. monocytogenes etiology, almost 90% were endogenous infections [8].
Factors contributing to the development of endogenous endophthalmitis include chronic diseases, particularly those associated with immunosuppression such as diabetes, cancer, hematological disorders, chronic kidney failure, post-organ transplant conditions, parenteral nutrition, long-term antibiotic treatment, steroid therapy, other immunosuppressive treatments, HIV infection, as well as advanced age or young age, especially in countries with low hygiene standards [1, 2, 4, 9]. In our patient, the predisposing factor for intraocular infection was IgG κ plasmocytic myeloma. A literature review indicates that patients with one or more immunosuppressive factors represented up to 37–47.5% of those with endogenous endophthalmitis caused by L. monocytogenes [8, 9].
Endogenous bacterial intraocular infection typically presents with an acute course, with the most common symptoms leading patients to seek ophthalmological consultation including decreased visual acuity (90%) and eye pain (50%), alongside complaints of injection of the eye, photophobia, and floaters in the field of vision [2, 10]. Physical examination reveals signs of inflammation, including hypopyon in the anterior chamber, posterior synechiae, vitreous exudation, and corneal edema [10]. Approximately one-third of patients with endophthalmitis caused by L. monocytogenes exhibit a symptom known as dark hypopyon, which results from iris necrosis and pigment dispersion [8]. In the case described, this distinctive symptom was not observed. However, it is important to recognize that it can also arise from intraocular infections of other etiologies or melanoma [8].
Blood cultures, which yield positive results in up to 75% of cases of endogenous endophthalmitis, play a crucial role in the diagnostic process [2]. Typically, cultures used to identify the specific pathogen involved are obtained from the aqueous humor or the vitreous body. Negative blood culture results could be attributed to transient bacteremia or fungemia, which may occur due to factors such as catheters, intravenous drug administration, or gastrointestinal endoscopic procedures [2]. The cause of the infection in our patient was verified by the findings of the anterior chamber fluid culture. Blood and vitreous cultures were negative. In patients with intraocular infections caused by L. monocytogenes, positive bacteriological results with identification of the causative microorganism were most frequently obtained from the aqueous humor (86% of cases), followed by the vitreous body (78%) and blood (23%) [9]. At present, the most sensitive method for diagnosing the cause of infectious endophthalmitis is polymerase chain reaction (PCR) analysis of a sample taken from the anterior chamber or vitreous body [11], though the procedure is not readily accessible.
The positive identification of L. monocytogenes in the anterior chamber fluid culture in our patient aligned with an above-normal elevation in monocyte count in the blood differential. An increase in monocytes is a hallmark of infection with this specific pathogen (hence its name – L. monocytogenes).
The management of endogenous endophthalmitis involves both intravitreal and intravenous administration of antibiotics. If a bacterial cause of infection is suspected, vancomycin (1 mg/0.1 ml) and ceftazidime (2.25 mg/0.1 ml) are commonly used empirically for local treatment with intravitreal injections [3]. Parenteral administration of antibiotics [2] should be started after collecting blood samples for culture [10]. In endogenous intraocular infections, the primary source of infection is located outside the eye, making systemic antibiotic therapy more appropriate compared to treatments for exogenous infections. Under normal physiological conditions, the blood-brain and blood-retinal barriers prevent most antibiotics from passing from the bloodstream into the tissues of the central nervous system and the eye [12]. In cases of endophthalmitis, the barrier is breached, allowing therapeutic drug levels to be achieved in the eye [9]. Similar to the approach used in the treatment of central nervous system infections, it has been proposed that administering high doses of antibiotics systemically can achieve effective drug concentrations in the vitreous body [14]. The treatment of choice in listeriosis is based on antibiotics from the penicillin group [15]. For confirmed cases of intraocular infections caused by L. monocytogenes, a combination of intravenous ampicillin and intravitreal vancomycin is recommended as the primary treatment approach [16]. In the reported case, after obtaining the intraocular culture results, we began treatment with intravenous ampicillin according to the antibiogram. A high daily dose, similar to that used for central nervous system infections, was administered. Additionally, intravitreal injections of vancomycin were maintained.
In severe instances of endogenous endophthalmitis, vitrectomy may be considered as a treatment option [2]. The procedure significantly reduces microorganisms and toxins in the vitreous body [10, 17], enhancing the chances of maintaining useful visual acuity and lowering the risk of evisceration or enucleation of the eye [2, 18]. It also allows for the collection of a vitreous body biopsy specimen for diagnostic purposes, which is particularly important when previous treatments have been ineffective [3]. In most cases where therapeutic vitrectomy was performed, it involved patients who had not responded to prior treatments or were at risk of vision loss [10].
In the case reported here, therapeutic vitrectomy was not conducted because the ultrasound showed inflammatory material firmly attached to the retinal surface, posing a high risk of mechanical damage to the retina during surgery. The patient described in this report regained full visual acuity without undergoing vitrectomy. The targeted systemic antibiotic therapy and intravitreal injections proved to be effective. Listeria monocytogenes demonstrates high susceptibility to penicillins [9]. Moreover, in this specific case, the time required to identify the causative agent and initiate targeted antibiotic treatment was relatively short (a few days). Nearly 40% of patients with endogenous endophthalmitis of this etiology end up with very poor visual acuity (less than 2/50) after treatment [8]. However, full recovery of vision is often possible. This is because endogenous blood-borne infections initially affect the choroid, and only later spread to the vitreous body and retina. In intraocular infections caused by L. monocytogenes, the initial sites of infiltration are the aqueous humor and vitreous body [9]. Consequently, in cases of endogenous endophthalmitis, the timeframe between diagnosis and the initiation of appropriate targeted treatment is of great importance for a successful outcome. In individuals with a possible immune deficiency who present with symptoms of uveitis, the primary diagnostic consideration should be endogenous endophthalmitis.
CONCLUSIONS
This report presents a case study of a patient with immunosuppression from multiple myeloma, who developed an endogenous intraocular infection of a rare etiology, caused by Listeria monocytogenes, and was successfully treated at the CMKP Department of Ophthalmology in Warsaw. To the best of our knowledge, this is the first such case reported in Polish ophthalmological literature.
However, given advancements in therapeutic techniques, such as contemporary immunosuppressive therapies and chemotherapy, which can facilitate endogenous intraocular infections, it is reasonable to expect a higher incidence of ocular complications of this nature. Ophthalmologists need to be mindful that endophthalmitis in immunocompromised patients that fails to respond to steroid treatment could be endogenous in nature, and that it might be the initial sign of a systemic infection that has spread from other organs through the bloodstream.