
 ENGLISH
ENGLISH





INTRODUCTION
Zoledronic acid is a widely used medication belonging to the group of bisphosphonates, which are a class of drugs inhibiting bone resorption prescribed primarily in osteoporosis and bone metastases. Bisphosphonates are notorious for their adverse effects, including ocular ones. They range from conjunctivitis, uveitis, episcleritis and scleritis to orbital inflammation [1, 2]. Other side effects are upper gastrointestinal tract adverse events (in the case of oral bisphosphonates), renal toxicity, acute phase response (manifesting as fever and flu-like symptoms), hypocalcaemia and secondary hyperparathyroidism, musculoskeletal pain, osteonecrosis of the jaw, atrial fibrillation, and atypical fractures of the femoral diaphysis [3].
A literature review from 2022 identified 101 reports [2] relating to bisphosphonate-associated ocular side effects. The mechanism of such complications may involve inhibition of farnesyl diphosphate (FPP) leading to both apoptosis of osteoclasts (the desired influence of these drugs) and intracellular accumulation of isopentenyl diphosphate (IPP) [3], resulting in activation of γ/δ T cells and release of cytokines [4], facilitating the inflammatory reaction after the bisphosphonate infusion.
In this article we aim to present a case of orbital inflammation, which was linked to recent infusion of zoledronic acid.
CASE REPORT
A 76-year-old man presented to the emergency department with left eye redness and eyelid swelling treated with chamomile compresses. His medical history included hypertension, hypothyroidism and prostate cancer with bone metastases, because of which 4 mg of zoledronic acid (brand name Osporil) had been administered three days before. Moreover, the patient had a record of cataract surgery and epiretinal membrane (ERM) in the right eye.
Best corrected visual acuity (BCVA) was 0.4 (Snellen) in the right eye, 0.5 in the left eye. Intraocular pressure (IOP) was 14 mmHg and 17 mmHg, respectively. Examination revealed eyelid oedema, conjunctival irritation and chemosis, cataract and pseudoexfoliation syndrome in the left eye. In the right eye, no pathologies were found in the anterior segment, while fundus examination confirmed the presence of ERM. Mild proptosis of the left eye was observed (exophthalmometry: right eye 18 mm, left 22 mm); therefore a computed tomography (CT) scan of the orbits was performed. It did not reveal any pathological changes. Since the eye movement was unlimited and the patient denied diplopia, an allergic reaction to chamomile was suspected. The patient was discharged with a prescription for topical corticosteroids.
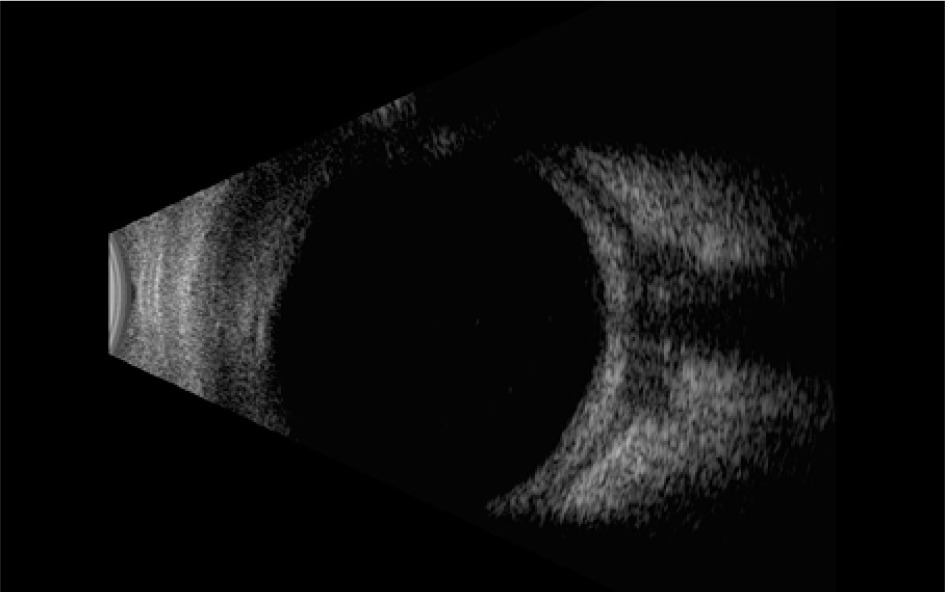
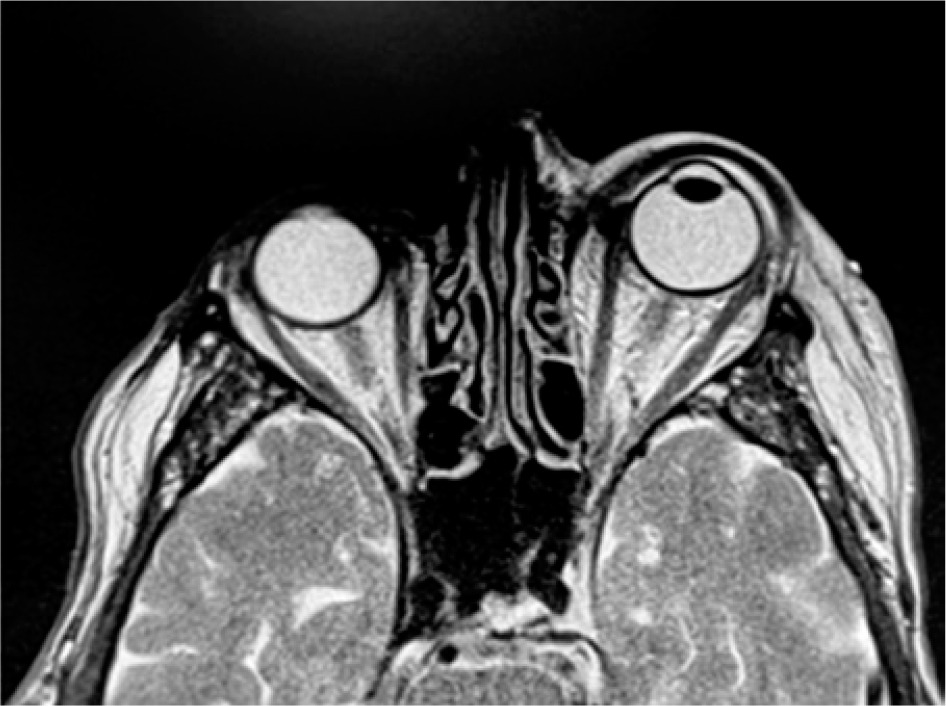
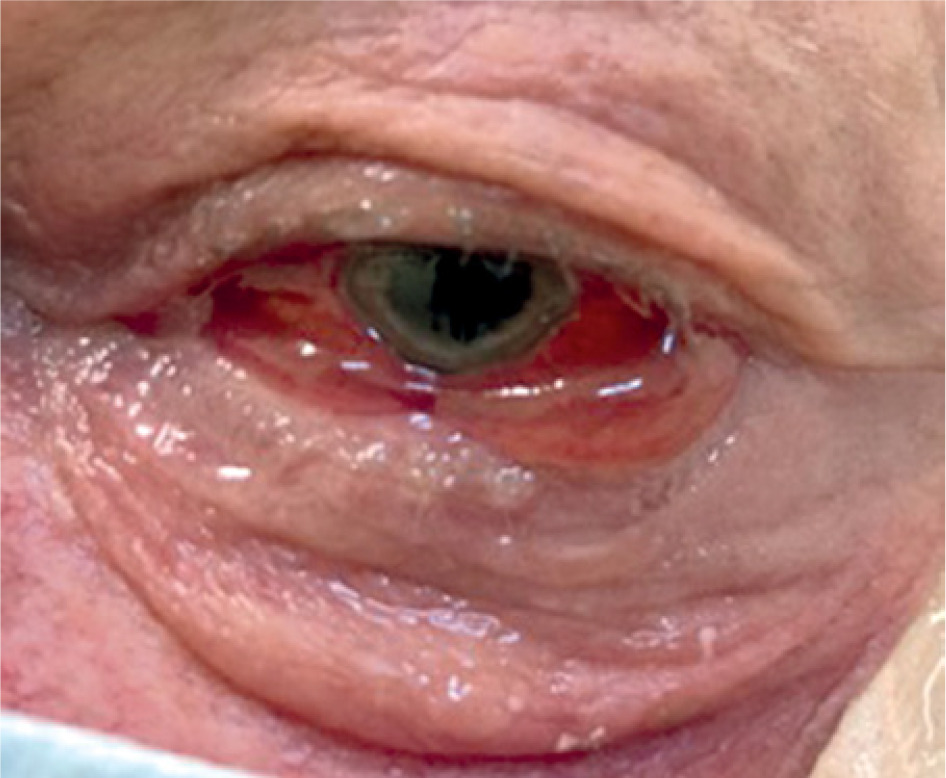
After 2 days the patient was again referred to the ophthalmological department due to severe deterioration. At the admission the BCVA in the left eye was hand motion, IOP 20 mmHg. The oedema increased, and conjunctival chemosis partially covered the swollen cornea (Figure 1). The motility of the eye was severely limited. Ultrasonography showed T-sign typical for scleritis (Figure 2). Within hours, IOP rose to 38 mmHg. Magnetic resonance imaging (MRI) of the orbits was performed (Figure 3). Moreover, conjunctival swabs were obtained.

Because zoledronate-induced orbital inflammation was suspected, intravenous (IV) methylprednisolone 0.5 g was administered along with acetazolamide and empirical antibiotics. The response to the steroid therapy was immediate: the following day the patient was able to count fingers from 1 metre. The ocular mobility was partially restored. The oedema was reduced, revealing signs of uveitis: irregular, non-reactive pupil with posterior synechiae, which were treated with mydriatics and topical steroids (Figure 4).
The patient received 3 doses of methylprednisolone and subsequently was switched to oral prednisone. Due to elevated blood pressure, the hypertensive therapy had to be intensified. After 8 days the patient was discharged with full recovery of visual acuity and normalised IOP. Apart from the oral prednisone taper, topical dexamethasone and moisturizing drops were prescribed.
The plausible severe adverse effect was reported to the Office for Registration of Medicinal Products, Medical Devices and Biocidal Products.
DISCUSSION
It is highly probable that this orbital inflammation was an adverse effect of zoledronic acid for two reasons. Firstly, the response to steroids was rapid. Secondly, there was an obvious time correlation between the drug administration and onset of the symptoms (typically within 1-7 days of an IV infusion) [2]. As hospitalization was required, it qualifies as a severe adverse event.
However, the differential diagnosis of orbital processes poses a challenge, and the sole term orbital inflammation is miscellaneous or, as some authors say, “generic”, [5] because it encompasses inflammatory pathologies of diverse aetiology, affecting various structures within the orbit.
Initially, orbital cellulitis could not be excluded; therefore antibiotics were given along with steroids.
The response to treatment with systemic corticosteroids is usually excellent [1, 6]. Spontaneous resolution of bisphosphonate-induced orbital inflammation is possible, but the administration of medication should not be delayed in severe cases due to the increased risk of further complications. In this case, the decision to implement intravenous methylprednisolone was based on the ineffectiveness of previous treatment with topical steroids, deep impairment of vision and the risk of irreversible ocular nerve neuropathy.
Nevertheless, systemic corticosteroids are also associated with numerous side effects [7] including for example immunodeficiency, hypertension, diabetes and osteoporosis, which is typically a pre-existing condition in patients receiving bisphosphonates. Consequently, it may be necessary to adjust the treatment of patients’ chronic diseases.
CONCLUSIONS
This case illustrates how numerous ocular complications of zoledronic acid may coincide, gradually affecting virtually all segments of the eye, thus leading to inflammation posing a threat of vision loss.
Given the ambiguity [2] of the recommendations concerning readministration of bisphosphonates after the occurrence of ocular side effects (many suggest that continuation of treatment is contraindicated [8], while some report uncomplicated rechallenge [9]), further research is needed.