
 POLSKI
POLSKI





INTRODUCTION
There are at least 2.2 billion cases of visual impairment or blindness worldwide, more than 1 billion of which result from lack of preventive measures or treatment. The number of blind children worldwide is about 1.4 million [1].
Experts estimate that 90% of people who are blind or visually impaired live in developing countries, with profound human and socio-economic consequences for low-income countries. The loss of productivity resulting from blindness and low vision, as well as the immediate costs for educating and rehabilitating these patients, has a serious impact on families, society and countries, especially those least able to bear such material costs. On the other hand, preventing and treating blindness using adequate and timely medical care can result in enormous savings for countries and support in development in a variety of ways [2]. One of the diseases leading to blindness is retinopathy of prematurity (ROP).
Retinopathy of prematurity is a severe disease affecting the retina of premature infants as a result of abnormal development of its vascular system. At later stages, fibrovascular proliferation leads to retinal detachment, visual impairment and, as a result, blindness. Each year, about 53,000 children suffer from severe forms of ROP that require timely laser treatment, and 20,000 children become blind or visually impaired [3]. Despite the fact that ROP is a preventable cause of blindness, this disease is still one of the leading causes of blindness and low vision in children worldwide. Ukraine is among countries where the risk of developing severe forms of ROP remains high. The only effective way to prevent blindness due to ROP is high-quality screening of premature babies, timely detection and treatment of ROP.
The aim was to develop a mobile model of ophthal- mological care for children with ROP in the Southern region of Ukraine, taking into account the available medical technologies, and study the effectiveness of its implementation.
MATERIAL AND METHODS
The Filatov Institute of Eye Diseases and Tissue Therapy of the National Academy of Medical Sciences of Ukraine is one of the first ophthalmological clinics in Ukraine where clinical experience in detection and treatment of children with ROP has been gained. Taking into account that in the Southern region of Ukraine there are 6 neonatal departments within a radius of 500 km where children with risk of severe ROP development are concentrated, a mobile group for timely identification and treatment of children with ROP was created in 2009 in the Institute. One of the main requirements was conducting screening examinations and treatment at the place of the child’s location.
The mobile group consisted of 2 ophthalmologists and 1 nurse. In Odesa, screening was conducted at the CNE Municipal Children’s Clinical Hospital No. 2 OCC and CNE Odesa Regional Children’s Clinical Hospital ORC at weekly intervals, to perform laser coagulation in the intensive care unit if necessary; in Mykolaiv, Kherson, Simferopol and Sevastopol, screening was conducted by local ophthal- mologists. When treatment was needed, a mobile team with the necessary equipment traveled from the institute to the city in question to perform laser coagulation.
In 2017, a project of the Filatov Institute together with the Nechytailo Family Foundation was organized as part of care for children with ROP, which allowed the quality of care for premature infants with ROP to be slightly improved. The foundation purchased a laser and a wide-angle retina camera for photo and video recording, as well as remote assessment of the severity of ROP, which allowed the decision to perform laser photocoagulation directly at the place of examination of children. The Foundation also provided a vehicle for systematic visits to screen children in Kherson and Mykolaiv.
In 2019, as part of the work in this area the Institute and Eye Samaritans International Charitable Foundation signed a memorandum of cooperation in the field of ROP. Thanks to Eye Samaritans International Foundation all ophthalmologists (Odesa, Kherson, Mykolaiv) involved in work with ROP were provided with modern binocular ophthalmoscopes, and the mobile group of the Institute was provided with a new laser system for ROP treatment. Eye Samaritans International Foundation is currently providing the running costs of transport rental to perform screening in neighboring regions. In the near future, Eye Samaritans International Foundation plans to equip intensive care units in Kherson and Mykolaiv with wide field retinal cameras.
According to the protocol for the treatment of ROP in Ukraine, premature infants with gestational age up to 37 weeks had to be examined. At the same time, the main risk group is children with a weight of up to 1,500 g and gestational age up to 32 weeks. The first screening examination of children was performed at 4 to 6 weeks after birth. Also, all preterm infants were screened immediately before discharge from the department regardless of their postconceptional age. The examination included reverse binocular ophthalmoscopy with a Keller head ophthalmoscope using aspheric lenses of 20 or 30 D and Barraquer soft blepharostats and sclerodepressors specially designed for newborns, including premature babies, after achieving effective mydriasis by instillation of a combination of cyclopentolate hydrochloride (1% Cyclomed) or tropicamide (1% tropicamide) and phenylephrine hydrochloride (2.5% Irifrine).
The frequency of follow-up examinations was determined by the ophthalmologist based on the results of the first examination. If ROP was not diagnosed at the examination, follow-up examinations were repeated every 2 weeks until the end of vascularization of zone 3 of the retina. If ROP was diagnosed, examinations were repeated weekly until the disease regressed on its own or reached a stage that required treatment. If any signs of ROP were detected, ocular fundus photo fixation was performed using a Panocam Visinex mobile wide-field digital pediatric camera (Panocam LT). If severe ROP was detected, the situation was discussed with specialists at the Institute remotely and a decision was made to carry out further treatment locally.
Indications for laser treatment were the following forms of the disease: aggressive ROP (A-ROP), formerly known as aggressive posterior retinopathy of prematurity (APROP), and pre-threshold ROP Type 1. Laser photocoagulation was performed under general anesthesia at the intensive care units of Odesa, Kherson and Mykolaiv regional hospitals (Republican Children’s Clinical Hospital of Simferopol, City Children’s Hospital of Sevastopol until 2014).
Vitra2 – a mobile laser system – was used to perform laser photocoagulation. The radiation power varied between 120 and 300 mW. The order of coagulation application was draining. The total number of coagulants during the operation reached 2,000 to 5,000 depending on the extent and severity of pathological changes on the ocular fundus.
Treatment efficacy was determined by improvement of the clinical picture of the ocular fundus (reduction and flattening of the proliferation shaft, reduction in the diameter and tortuosity of the vessels of the posterior pole of the eye), which meant regression or stabilization of the pathological process. A center for prevention of childhood blindness as a result of ROP was established at the Institute through the joint efforts of the Nechytailo Foundation as well as Eye Samaritans International, which monitors the condition of postoperative children, as well as the long-term results of ROP treatment and the natural course of self-regressed ROP in older children.
RESULTS
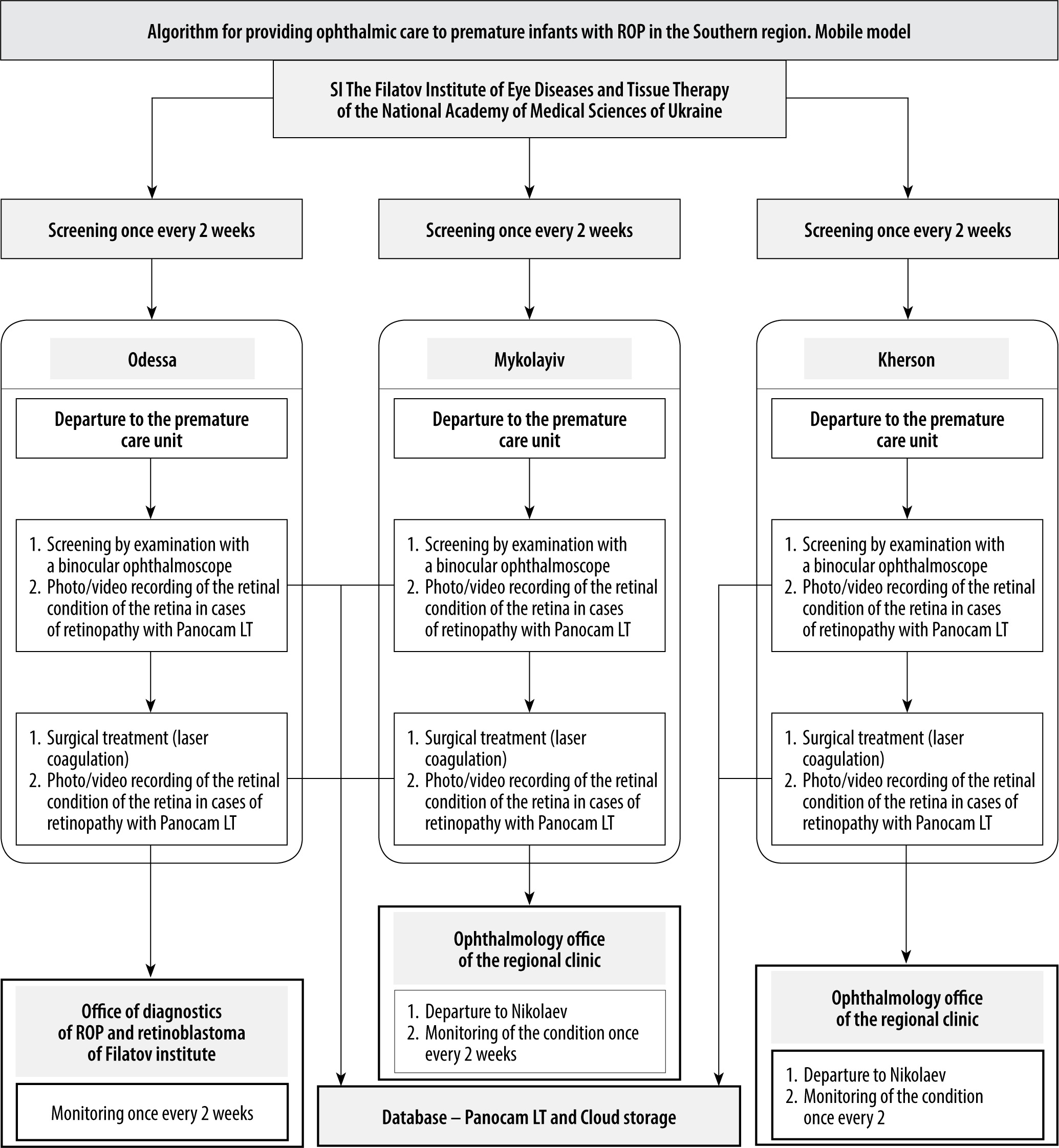
A mobile model of ophthalmological care for premature babies in the Southern region of Ukraine has been developed; its stepwise algorithm is shown in Figure 1.
Figure 1
Algorithm of ophthalmological care for premature infants with ROP in the Southern region. The Mobile model
A multidisciplinary team of specialists for the care of prematurely born children with ROP, including neo- natologist, anesthesiologist-resuscitator, pediatric ophthal- mologist and nurses, was created, with the participation of the Institute, at the specialized department for the care of prematurely born children in children’s hospitals. If neces- sary, a psychologist, doctors of other specialties and social workers are involved.
The main tasks of the multidisciplinary team are: regulation of interactions between neonatology, intensive care and ophthalmology services; development of complex recommendations for the child’s care; preparation of recommendations for further management and monitoring of the child upon discharge; preparation of recommendations for the family (legal representatives) on the child’s needs, required assistance and specifics of his/her home care upon discharge.
Work with parents of a prematurely born child with ROP is carried out continuously, at all stages, involving members of the multidisciplinary team for the care of prematurely born children with ROP, depending on the required competence. Work with parents includes: providing information on the specifics of care for a premature baby, the need for examination of the premature baby and the threat of ROP development, the child’s diagnosis and treatment options, rehabilitation options for the disease; provision of psychological and social assistance; explanation of recommendations on the child’s needs, necessary assistance and features of home care for the child.
As a result, in the period 2009-2021, 5,516 prematurely born children were examined within the developed mobile model of ophthalmological care, who underwent 15,450 screenings: in Odesa region – 4,902 children (14,228 screenings); in Mykolaiv region – 279 children (740 screenings); in Kherson region – 294 children (441 screenings); in Crimea (until 2014) – 41 children (41 screenings).
711 telemedicine consultations by means of Panocam LT (Visinex): in Odesa region – 269; in Mykolaiv region – 200; in Kherson region – 242.
Laser treatment of 423 children was performed from 2009 to 2021: 197 children in Odesa region, 90 children in Mykolaiv region, 95 children in Kherson region, and 41 children in Crimea (until 2014). Regression of the disease due to retinal laser photocoagulation was observed in 407 children (96.2%). In 16 children (3.8%), the disease progressed to stages IV-V of ROP, which required further vitreoretinal intervention: in Odesa region – 7 children, in Mykolaiv region – 6 children, in Kherson region – 3 children.
Analysis of the results of ophthalmological examination of children showed that during the whole period of obser- vation different stages of ROP were diagnosed in 1,440 out of 5,516 preterm born children (26.1%). At the same time in 423 children (7.6%) progression of ROP was registered that required laser treatment.
Over the entire period of work, the mobile team made 1,672 visits to conduct screening examinations, telemedicine consultations and laser photocoagulation of premature newborns, of which 1,377 visits to the City Clinical Hospital and Odesa Regional Clinical Hospital were made, 121 visits to the Mykolaiv Regional Clinical Hospital, 133 visits to the Kherson Regional Clinical Hospital, 41 visits to the Crimea (until 2014).
All data are presented in Table I.
Table I
Number of visits, examined children, screenings, telemedicine consultations, laser photocoagulation and patients referred for vitreoretinal intervention for 2009-2021
The positive treatment results obtained testify to the high clinical effectiveness of the developed model of care for premature infants, which serves as a prerequisite for the prevention of the development of severe ROP-related complications and blindness.
In addition, it was confirmed that laser treatment of a prematurely born child with ROP in the hospital setting at the place of his stay has a positive impact on health of the child, who, due to the presence of associated prematurity disorders of physiological functions, is prone to a high risk of developing various disorders of vital functions. The main advantages of this format are elimination of risks associated with transportation of the oxygen-dependent child to the ophthalmic clinic and the possibility of using telemedicine tools.
For the first time in practice of ophthalmological care for premature infants with ROP or at risk of its development, a multidisciplinary and family-oriented approach was introduced into the system, which provided comprehensive multidisciplinary care for the child and his family. Only with close interaction among different specialists and an integrated approach to the problem of care for a preterm infant with ROP can we expect good treatment results and subsequently improved quality of life of this population of children.
DISCUSSION
According to the World Health Organization (WHO), about 15,000,000 children are born prematurely in the world annually, that is more than 10% of all born children [4]. In Ukraine, about 20,000 premature babies are born annually, among them about 1000 children with extremely low birth weight (less than 1,000 g) [5, 6].
Breathing and rehabilitation of premature infants is a complex process that lasts for months and is characterized by a high risk of various complications and diseases [7-9]. Many premature infants who survive have disabilities. Over- all, according to a meta-analysis, the frequency of neuro- sensory disability among extremely premature infants in the developed countries ranges from 10.9% to 26.8%, while among preterm infants the range is 0.1-2.3% [10, 11].
That is why in 2014 Ukraine joined the Global Every Newborn Action Plan by the WHO [11], which aims to reduce the number of preventable deaths and the incidence of severe pathology in newborns.
One of the most severe diseases affecting preterm infants is ROP, which, according to various literary sources, develops in 10-66% of preterm infants [13, 14]. The significant variation in the prevalence of ROP is primarily due to the different definitions of the risk group for ROP development among newborns by gestational age and birth weight in different countries [13]. For example, this percentage is slightly higher in South-East Asia and Latin America. The prevalence of the disease among Europeans and African Americans is almost the same, but progression to severe forms is more common among the “white” European race. It has also been observed that, compared with female infants, male infants are more frequently affected by the disease [14].
The incidence of blindness due to ROP varies worldwide depending on the degree of development of society, the level of neonatal care, as well as the timely diagnosis and treatment of the disease in a particular country. In highly developed countries, this rate does not exceed 8%, while in developing countries it is 40%, reaching 60% in some regions [15, 16].
Babies with a low birth weight (1,000-1,499 g) or very low birth weight (500-999 g) are the most vulnerable among premature infants. For example, children with a birth weight of less than 800 g have an incidence of ROP of up to 90% [8, 17-19].
According to the official data of the Center of Medical Statistics of the Ministry of Health of Ukraine, ophthalmic pathology takes fourth place (5.25%) in the structure of all human diseases. The number of children with disabilities due to diseases of the eye and appendage apparatus is about 3-4% of the total number of children with disabilities [5].
Approximately 80% of cases of ROP undergo spontaneous regression without special interventions [9, 18, 19]. But about 20% of people, who statistically have progression of the disease, are at risk of irreversible blindness without timely treatment. They are the ones who annually “join” visually impaired people from early childhood. Therefore, the issue of providing children with ROP with the most qualitative care in order to have an opportunity to become full-fledged members of society in future should remain a priority for the state. The most important task today is to conduct timely screening of all premature babies in the risk group for the development of ROP.
Recently, telemedicine as a segment of health care has become increasingly popular in the world. This type of counseling is particularly promising in the case of prematurely born babies. This is due to the fact that premature babies are poorly transportable because of associated physiological abnormalities. Their transfer to another medical facility, even with an intensive care team vehicle, is often life-threatening. Most programs using telemedicine devices in the United States, Germany and Canada are performed by nurses or ophthalmologists. At the same time, many countries have a shortage of ROP specialists, which leads to untimely diagnosis and delayed initiation of treatment, resulting in lost time in providing the right ophthalmic care and preserving the child’s vision. As a rule, interpretation of the results takes place either on the spot (in the case of photo-registration performed by an ophthalmologist) or remote by ROP “experts” (in the case of photo-registration performed by junior or non-medical staff) during a certain period. The evaluation period for photographs can vary from a few hours to a week. However, studies show that photographic documentation can “unintentionally” detect the initial stage of the disease that was “missed” during the ophthalmoscopic examination [20]. Thus, the ability to document, view, store and compare images greatly exceeds the effectiveness of conventional indirect ophthalmoscopy. Given the shortage of specialists skilled in binocular ophthalmoscopy, telemedicine can improve the availability of ROP screening in developing countries, including Ukraine.
In 2003 in Canada, Ells et al. evaluated the use of distal digital retinal photo-reading using the RetCam-120 (Massie Research Laboratories Inc., Dublin, CA) in the diagnosis of 44 patients with severe ROP. Photoregistration of ocular fundus structures was performed by a healthcare professional. Indirect ophthalmoscopy was also performed in all patients. In the case of detection of severe stages of ROP requiring treatment (23 eyes), the sensitivity of the digital method was 100%, specificity 96%. The positive predictive value of the digital diagnostic method was 92% and the negative predictive value was 100%. In 87% of cases, severe ROP was diagnosed using telemedicine before or simultaneously with specialists performing indirect ophthalmoscopy [21].
Colleagues from Germany also described their 6-year experience of applying a telemedicine screening program in a group of 1,222 preterm infants, in which wide-angle digital cameras (RetCam 120, Massie Lab, Pleasanton, California, USA) were installed in five neonatal intensive care units in Germany. Photoregistration of ocular fundus structures (6 images for each eye) and binocular ophthalmoscopy were performed for all preterm infants according to German recommendations of ophthalmologists. The image data were coded and transmitted to the Reading Center in Regensburg for evaluation. The sensitivity for identifying ROP requiring treatment was 100% and the positive predictive value was 82.4% (28/34). Thus, all cases of severe ROP were detected in time [22].
Stanford University presented a one-year experience of using telemedicine technology to diagnose ROP. According to that study, 42 children (84 eyes) with ROP were examined with the RetCam II (1,315 images) and evaluated by the SUNDROP Reading Center at Stanford University. The examination was performed by junior medical staff and 5 photographs were taken for each eye. Sensitivity and specificity were 100% and 95%, respectively. No cases of ROP were missed during the 12-month follow-up period [23].
Internet Diagnosis of Retinopathy of Prematurity (KIDROP) in Karnataka, India is the largest tele-ophthalmology program of the Narayana Netralaya Institute of Post-graduate Education, in which the aim is for preterm infants to be examined by a non-medical person (technician) for ROP in remote areas using the Retcam Shuttle (Clarity MSI, USA) – a large format digital imaging device. Thanks to state and private sector funding, the number of neonatal centers covered by KIDROP has increased from 3 to 81 since 2008. KIDROP is based on the “triple T” philosophy: telemedicine, training of ophthalmologists, and talking to neonatologists, pediatricians and gynecologists. KIDROP trains technicians for infant screening in neonatal centers located in the periphery, where there are no ophthalmologists skilled in indirect ophthalmoscopy. Technician training and certification is conducted according to a developed training methodology with a scoring system that is used to accredit a novice technician at different skill levels (Level I, II and III). Assessment parameters include basic knowledge of the disease and program; the technician’s ability to obtain well-focused, oriented images in the correct sequence; the speed of the procedure; the ability to evaluate the image and establish a diagnosis; and the technician’s ability to upload and process photos. The diagnosis is made using a template created by KIDROP, according to which the patient is sorted into a group depending on the diagnosis: the “red” group – with ROP Type 1 or severe ROP in one or both eyes, which needs treatment or urgent expert evaluation; the “orange” group – with ROP Type 2 in at least one eye, which needs follow-up care; the “green” group – children who no longer need to be examined. In addition, KIDROP has created a hardware and software platform (Tele-Care [i2i Telesolutions]) with patented photo compression technology that allows real-time downloading of photos and their viewing by a remote examiner on a device (iPhone, iPad, personal computer) using an app (Apple, CA, USA) anywhere in the world.
The mobile team usually consists of 3-4 people: a manager, 1-2 technicians and a driver. Each team covers 16-28 neonatal centers in Karnataka State on a weekly basis. The radius from the main center is approximately 300 km. Managers serve as a liaison between the neonatal center doctors and the mobile team. Managers inform mothers about the importance of follow-up examinations, schedule visits and record data from the screening session. In turn, technicians operate the equipment, i.e. a portable retinal camera (Retcam Shuttle) and a laptop equipped with a software system, perform photo- registration of the eye fundus structures and evaluate taken photos. A remote expert performs photo assessment in cases where it is necessary, taking into account the technician’s level of training [24].
KIDROP is the largest non-medical program in the world. Vinecar et al. studied the effectiveness of KIDROP by analyzing 6,339 imaging sessions of 1,601 children. According to the results of the study, a level III specialist agreed with 94.3% of all expert decisions. The sensitivity, specificity, positive and negative predictive values for ROP requiring treatment were 95.7, 93.2, 81.5, and 98.6%, respectively. Only 0.4% of children requiring treatment were missed [25].
Disadvantages of helping premature children with ROP in Ukraine are primarily the lack of ophthalmologists, as well as the fact that in most regions children often need additional consultation with a specialist in ROP. It should be noted that retinal laser photocoagulation in premature babies at their place of residence is not possible in all regions, which in some cases makes it difficult to perform laser intervention in a timely manner. In general, children are transported to the National Children’s Hospital Okhmatdet for treatment and it may be unsafe for their general condition.
The mobile model of ophthalmological care proposed by us implies screening and laser intervention directly at the place of the child’s location. It should also be noted that the use of telemedicine technologies in our case makes it possible to organize real-time transmission of images of ocular fundus of a newborn child at risk of ROP development to the Institute. Consequently, an expert without wasting time can help to decide on making an accurate diagnosis and determining the tactics of managing a patient with ROP. Taking into account that the photo-registration procedure is performed by a qualified ophthalmologist, laser intervention is possible on the day of examination, if necessary.
The established mobile model of ophthalmological care for premature babies has made it possible to reduce the number of children with disabilities due to ROP. To date, the Institute has organized a center for the prevention of infant blindness, which mainly monitors children with ROP.
Thus, only with close interaction between different specialists and an integrated approach to the problem of care for a premature infant with ROP can we expect better treatment results and improved quality of life of such children.
CONCLUSIONS
It has been established that the developed mobile model of ophthalmological care for premature babies in the Southern region of Ukraine makes it possible to provide a full cycle of diagnostic and therapeutic measures for premature babies with ROP, in different stages of the disease, due to the continuity of organizational stages of ophthalmological care: active early screening, telemedicine consultation, timely and highly accurate treatment of ROP, dynamic monitoring, involvement of allied professionals and parents of the child in the treatment process.
The high efficiency of the developed mobile model of ophthalmological care was established due to the increase in the percentage of early detection of ROP in premature infants and achievement in them of good functional indicators after laser photocoagulation – incidence of ROP among premature infants – 26.1%; incidence of ROP requiring treatment – 7.6%; overall treatment efficiency – 96.2%.
For the first time a multidisciplinary and family-oriented approach was introduced into the practice of ophthalmological care for premature infants with ROP or at risk of ROP development, which provided comprehensive multidisciplinary care for the child and his/her family due to regulation of interactions between neonatological, intensive care and ophthalmological services, and compliance with the continuity of stages of medical care for premature infants.
The developed mobile model of ophthalmological care for premature babies in the Southern region of Ukraine makes it possible to improve the work of the preventive direction of the regional health care system by applying active screening methods of early diagnosis of ROP and thereby reduce cases of partial and complete loss of vision for the child population of the region.